
Autonomic/CV Drugs — MCQs

On this page
A 28-year-old woman with a history of migraines presents to your office due to sudden loss of vision in her left eye and difficulty speaking. Two weeks ago she experienced muscle aches, fever, and cough. Her muscle aches are improving but she continues to have a cough. She also feels as though she has been more tired than usual. She had a similar episode of vision loss 2 years ago and had an MRI at that time. She has a family history of migraines and takes propranolol daily. On swinging light test there is decreased constriction of the left pupil relative to the right pupil. You repeat the MRI and note enhancing lesions in the left optic nerve. Which of the following is used to prevent progression of this condition?
A 30-year-old woman is brought to the emergency department because of a 30-minute history of palpitations, dizziness, and chest discomfort. She has also not urinated since she woke up. She has a history of fibromyalgia treated with clomipramine. There is no family history of serious illness. She does not smoke or drink alcohol. Her temperature is 37°C (98.6°F), pulse is 120/min, and blood pressure is 90/60 mm Hg. On mental status examination, she is confused. Examination shows dilated pupils and dry skin. The abdomen is distended, there is tenderness to deep palpation of the lower quadrants with no guarding or rebound and dullness on percussion in the suprapubic region. An ECG shows tachycardia and a QRS complex width of 110 ms. Activated carbon is administered. The patient is intubated. Intravenous fluids and oxygenation are begun. Which of the following is the most appropriate pharmacotherapy for this patient?
A patient is receiving daily administrations of Compound X. Compound X is freely filtered in the glomeruli and undergoes net secretion in the renal tubules. The majority of this tubular secretion occurs in the proximal tubule. Additional information regarding this patient's renal function and the renal processing of Compound X is included below: Inulin clearance: 120 mL/min Plasma concentration of Inulin: 1 mg/mL PAH clearance: 600 mL/min Plasma concentration of PAH: 0.2 mg/mL Total Tubular Secretion of Compound X: 60 mg/min Net Renal Excretion of Compound X: 300 mg/min Which of the following is the best estimate of the plasma concentration of Compound X in this patient?
A 37-year-old female presents to the emergency room complaining of headaches and palpitations. She reports that she initially started experiencing these symptoms several months prior but attributed them to stress at work. The symptoms occur episodically. Her family history is notable for medullary thyroid cancer and hyperparathyroidism. Her temperature is 98.6°F (37°C), blood pressure is 165/90 mmHg, pulse is 105/min, and respirations are 18/min. On examination she appears tremulous. Urine metanephrines are elevated. Which of the following is the most appropriate first medication in the management of this patient’s condition?
A 28-year-old woman, gravida 1, para 0, at 32 weeks' gestation is evaluated for vaginal bleeding. Five days ago, she was admitted to the hospital and started on treatment for a deep vein thrombosis in the right leg. Her pulse is 125/min and blood pressure is 95/67 mm Hg. Physical examination shows large hematomas on the upper limbs and swelling in the right calf. There is a large amount of bright red blood in the vaginal vault. Laboratory studies show a hemoglobin of 8.9 mg/dL, platelet count of 185,000/mm3, and activated partial thromboplastin time of 160 seconds. Which of the following is the most appropriate pharmacotherapy to rapidly reverse this patient's coagulopathy?
A 30-year-old man presents to your clinic complaining of excessive thirst and frequent urination for the past few months. Urine testing reveals a low urine osmolarity, which fails to increase after subjecting the patient to a water deprivation test and injection of desmopressin. Further into the encounter, the patient reveals that he has been on a mood stabilizer for bipolar disorder for several years. Which of the following is the most likely cause of his polyuria?
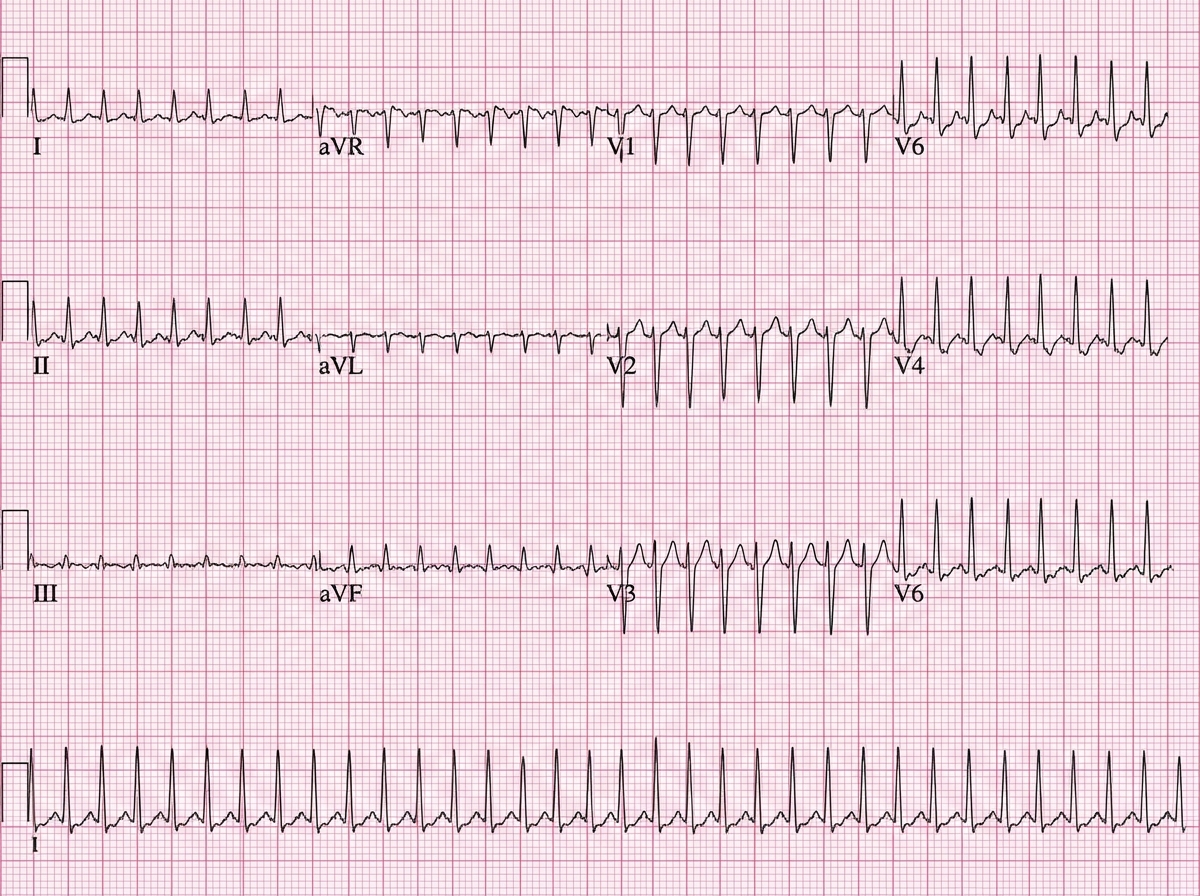
A 52-year-old man presents to the emergency department (ED) complaining of palpitations and lightheadedness for the last 30 minutes. He denies feeling pain or discomfort in his chest and is not short of breath. He does not have any known medical problems and does not take any medications regularly. He drinks 4–6 caffeinated drinks a day. The temperature is 36.8°C (98.2°F), the pulse rate is 150/min and slightly irregular, the blood pressure is 144/84 mm Hg, and the respiratory rate is 16/min. A focused examination of the cardiovascular and respiratory systems is unremarkable. An electrocardiogram is performed in the ED and the results are shown in the accompanying image. The ED physician prescribes a calcium channel blocking agent for his condition. Which of the following statements best describes the choice of verapamil over nifedipine in the treatment of this patient?
A 69-year-old man with type 2 diabetes mellitus comes to the physician for a follow-up examination. His only medication is metformin. He has tried to lose weight for several years without success. He is 168 cm (5 ft 6 in) tall and weighs 110 kg (243 lb); BMI is 39 kg/m2. His hemoglobin A1c is 8.5%. Which of the following is the most appropriate antidiabetic drug to address both this patient's glucose control and weight?
A 42-year-old man comes to the physician because of a 6-month history of progressively worsening shortness of breath with exertion. He was diagnosed with systemic sclerosis 5 years ago. Vital signs are within normal limits. Physical examination shows puffy, taut skin over the fingers. Pulmonary examination is unremarkable. There is no jugular venous distention. An x-ray of the chest shows enlargement of the pulmonary vessels and a prominent right heart border. Cardiac catheterization shows elevated right ventricular pressures and a mean pulmonary artery pressure of 55 mm Hg. Treatment with tadalafil is begun. The expected beneficial effect of this drug is most likely due to which of the following actions?
A 55-year-old man with a history of repeated hospitalization for chronic pancreatitis comes to the physician because of difficulty walking and standing steadily. Neurological examination shows an unsteady, broad-based gait, distal muscle weakness, decreased deep tendon reflexes, and an abnormal Romberg test. His hemoglobin concentration is 11.9 g/dL, mean corpuscular volume is 89/μm3, and serum lactate dehydrogenase is 105 U/L. His serum haptoglobin is slightly decreased. A deficiency of which of the following substances is the most likely cause of this patient's findings?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app