
Antivirals — MCQs

On this page
A 65-year-old man presents to a clinic after 2 days of pain just below the right nipple. The pain radiates to the scapula. The rash was preceded by a burning and tingling pain in the affected region. His medical history is relevant for hypertension and hypercholesterolemia. He does not recall his vaccination status or childhood illnesses. A physical examination reveals stable vital signs and a vesicular rash distributed along the T4 dermatome. Which of the following is most appropriate for treating his condition and preventing further complications?
A 27-year-old woman presents with painful swallowing for the past 2 days. She received a kidney transplant 3 months ago for lupus-induced end-stage renal disease. She takes tacrolimus, mycophenolate mofetil, prednisone, and calcium supplements. The blood pressure is 120/80 mm Hg, the pulse is 72/min, the respirations are 14/min, and the temperature is 38.0°C (100.4°F). Esophagoscopy shows serpiginous ulcers in the distal esophagus with normal surrounding mucosa. Biopsy shows large cytoplasmic inclusion bodies. Which of the following is the most appropriate pharmacotherapy at this time?
A 31-year-old man with untreated HIV infection is admitted to the hospital because of a 3-day history of blurred vision and flashing lights in his left eye. Indirect ophthalmoscopy shows retinal hemorrhages of the left eye. Treatment with a drug that directly inhibits viral DNA polymerases by binding to pyrophosphate-binding sites is initiated. Two days later, the patient has a generalized tonic-clonic seizure. This patient's seizure was most likely caused by which of the following?
A 29-year-old female presents to her gynecologist complaining of a painful rash around her genitals. She has multiple sexual partners and uses condoms intermittently. Her last STD screen one year ago was negative. On examination, she has bilateral erosive vesicles on her labia majora and painful inguinal lymphadenopathy. She is started on an oral medication that requires a specific thymidine kinase for activation. Which of the following adverse effects is associated with this drug?
A 27-year-old man presents to the family medicine clinic for a routine check-up. The patient recently accepted a new job at a childcare center and the employer is requesting his vaccination history. After checking the records from the patient’s childhood, the physician realizes that the patient never had the varicella vaccine. The patient is unsure if he had chickenpox as a child, and there is no record of him having had the disease in the medical record. There is no significant medical history, and the patient takes no current medications. The patient’s heart rate is 82/min, respiratory rate is 14/min, temperature is 37.5°C (99.5°F), and blood pressure is 120/72 mm Hg. The patient appears alert and oriented. Auscultation of the heart reveals no murmurs, rubs, or gallops. The lungs are clear to auscultation bilaterally. With regard to the varicella vaccine, which of the following is recommended for the patient at this time?
A 9-month-old boy is brought to a pediatrician by his parents for routine immunization. The parents say they have recently immigrated to the United States from a developing country, where the infant was receiving immunizations as per the national immunization schedule for that country. The pediatrician prepares a plan for the infant’s immunizations as per standard US guidelines. Looking at the plan, the parents ask why the infant needs to be vaccinated with injectable polio vaccine, as he had already received an oral polio vaccine back in their home country. The pediatrician explains to them that, as per the recommended immunization schedule for children and adolescents in the United States, it is important to complete the schedule of immunizations using the injectable polio vaccine (IPV). He also mentions that IPV is considered safer than OPV, and IPV has some distinct advantages over OPV. Which of the following statements best explains the advantage of IPV over OPV to which the pediatrician is referring?
A thymidine kinase-deficient varicella-zoster virus strain has been isolated at a retirement home. Many of the elderly had been infected with this strain and are experiencing shingles. Which of the following would be the best antiviral agent to treat this population?
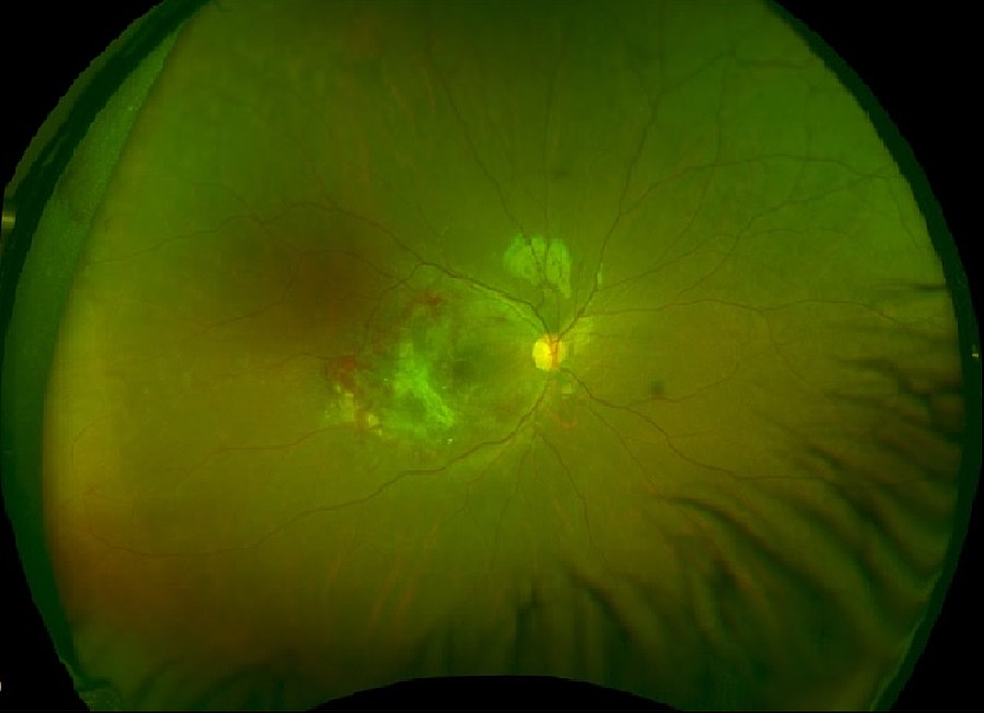
A 40-year-old man presents with problems with his vision. He says he has been experiencing blurred vision and floaters in his left eye for the past few days. He denies any ocular pain, fever, or headaches. Past medical history is significant for HIV infection a few years ago, for which he is noncompliant with his antiretroviral medications and his most recent CD4 count was 100 cells/mm3. His temperature is 36.5°C (97.7°F), the blood pressure is 110/89 mm Hg, the pulse rate is 70/min, and the respiratory rate is 14/min. Ocular exam reveals a decreased vision in the left eye, and a funduscopic examination is shown in the image. The patient is admitted and immediately started on intravenous ganciclovir. Despite completing adequate induction therapy, he develops dose-limiting myelosuppression, so he is switched to a different medication. Inhibition of which of the following processes best describes the mechanism of action of the newly added medication?
A 65-year-old male is evaluated in clinic approximately six months after resolution of a herpes zoster outbreak on his left flank. He states that despite the lesions having resolved, he is still experiencing constant burning and hypersensitivity to touch in the distribution of the old rash. You explain to him that this complication can occur in 20-30% of patients after having herpes zoster. You also explain that vaccination with the shingles vaccine in individuals 60-70 years of age can reduce the incidence of this complication. What is the complication?
A 45-year-old man presents for follow-up to monitor his chronic hepatitis C treatment. The patient was infected with hepatitis C genotype 1, one year ago. He has been managed on a combination of pegylated interferon-alpha and ribavirin, but a sustained viral response has not been achieved. Past medical history is significant for non-alcoholic fatty liver disease for the last 5 years. Which of the following, if added to the patient’s current treatment regimen, would most likely benefit this patient?
Practice by Chapter
HIV protease inhibitors
Practice Questions
HIV reverse transcriptase inhibitors
Practice Questions
HIV integrase inhibitors
Practice Questions
HIV entry inhibitors
Practice Questions
Hepatitis B antivirals
Practice Questions
Hepatitis C direct-acting antivirals
Practice Questions
Influenza antivirals
Practice Questions
Herpesvirus antivirals
Practice Questions
Cytomegalovirus antivirals
Practice Questions
Respiratory syncytial virus therapies
Practice Questions
Broad-spectrum antivirals
Practice Questions
Antiretroviral resistance
Practice Questions
Antiviral prophylaxis strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app