
Antivirals — MCQs

On this page
A 20-year-old man is brought to the emergency department for evaluation of an animal bite. He was hiking earlier that day when he was bitten by a raccoon. He says the attack was unprovoked and the animal ran away after the encounter. He was bitten by a stray dog when he was 11 years old and received postexposure prophylaxis for rabies at that time. His immunizations are up-to-date. His immunization record shows he received 3 doses of diphtheria-tetanus-acellular pertussis vaccine as a child and a tetanus-diphtheria-acellular pertussis vaccination at the age of 16. He is in no apparent distress. His temperature is 98.4°F (36.9°C), pulse is 72/min, respirations are 18/min, and blood pressure is 124/75 mm Hg. He has a wound on his left lower extremity with actively bleeding puncture sites. The wound is thoroughly irrigated with normal saline and cleansed with antiseptic and a bandage is applied. Which of the following is the most appropriate next step in management?
A 30-year-old woman presents with generalized fatigue, joint pain, and decreased appetite. She says that symptoms onset a year ago and have not improved. The patient’s husband says he has recently noticed that her eyes and skin are yellowish. The patient denies any history of smoking or alcohol use, but she admits to using different kinds of intravenous illicit drugs during her college years. The patient is afebrile and vital signs are within normal limits. Physical examination is unremarkable, except for moderate scleral icterus. A polymerase chain reaction (PCR) of a blood sample is positive for a viral infection that reveals a positive-sense RNA virus, that is small, enveloped, and single-stranded. The patient is started on a drug that resembles a purine RNA nucleotide. She agrees not to get pregnant before or during the use of this medication. Which of the following is the drug that was most likely given to this patient?
A 31-year-old man comes to the emergency department because of drooping of the left side of his face since awakening that morning. He had difficulty chewing his food at breakfast. He was treated the previous day at the hospital after sustaining a head injury from falling off a ladder while working on his roof. A plain CT of the brain at that visit showed no abnormalities. He is in no apparent distress. His vital signs are within normal limits. The pupils are equal and reactive to light. There is drooping of the left corner of the mouth. The left nasolabial fold is flattened. When asked to close both eyes, the left eye remains partially open. There are no wrinkles on the left side of the forehead when the eyebrows are raised. Which of the following is the most appropriate next step in management?
A 24-year-old woman with HIV infection comes to the physician for a follow-up examination. She has been inconsistently taking combined antiretroviral therapy for the past 5 years. She did not receive any childhood vaccinations because her parents were against them. During the consultation, the patient says that she wants to catch up on the missed vaccinations. Laboratory studies show a CD4+ T lymphocyte cell count of 180/mm3. Administration of the vaccine against which of the following agents should be avoided in this patient?
A 28-year-old woman presents to the emergency department with a sudden onset of nausea, vomiting, and pain in the upper abdomen for the past 3 hours. She reports that the pain has increased in severity over these 3 hours and frequently radiates to the back. She was diagnosed as HIV positive 2 years ago. She was placed on raltegravir/tenofovir/emtricitabine 1 year ago, but because of treatment failure, her antiretroviral therapy was changed to abacavir/didanosine/dolutegravir/enfuvirtide/fosamprenavir 3 months ago. Her temperature is 37.8°C (100.0°F), heart rate is 110/min, respiratory rate is 18/min, and blood pressure is 124/80 mm Hg. Abdominal examination shows tenderness in the upper abdomen, but there is an absence of guarding or rigidity. Ultrasonography of the abdomen shows an edematous pancreas and an absence of gallstones. Laboratory studies show: Serum glucose 120 mg/dL Serum aspartate aminotransferase 74 U/L Serum alanine aminotransferase 88 U/L Serum amylase 800 U/L Serum triglyceride 125 mg/dL In addition to pain control, which of the following is an appropriate initial step in treatment?
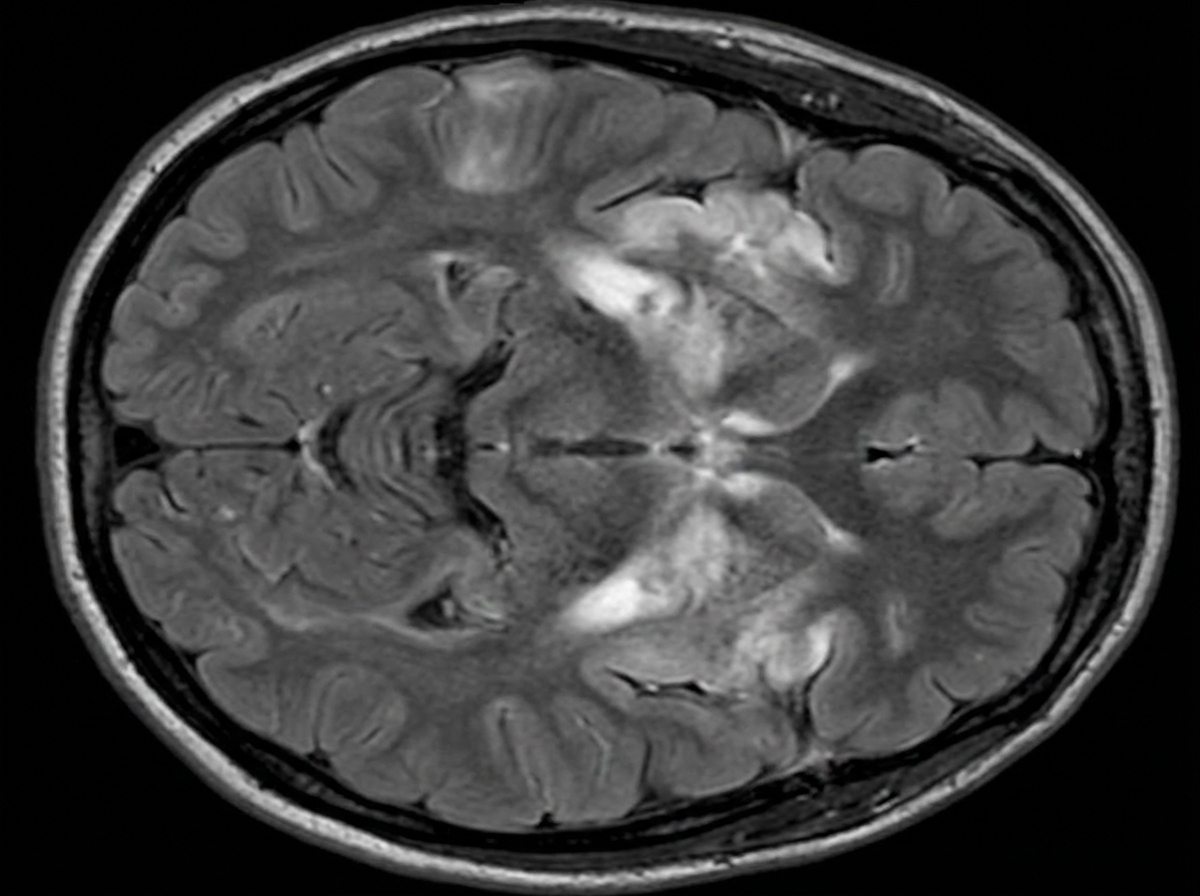
A 46-year-old man is brought to the emergency department because of worsening confusion and weakness in his right arm and leg for 2 days. He has also had fever and headache that began 5 days ago. He has hypertension and type 2 diabetes mellitus. Current medications include metformin and lisinopril. His temperature is 39.3°C (102.7°F), pulse is 103/min, and blood pressure is 128/78 mm Hg. He is confused and agitated. He is not oriented to person, place, or time. Neurologic examination shows nuchal rigidity. Muscle strength is 3/5 on the right upper and lower extremity strength but normal on the left side. His speech is incoherent. An ECG shows no abnormalities. An MRI of the brain is shown. Shortly after the MRI scan, the patient has a seizure and is admitted to the intensive care unit following administration of intravenous lorazepam. Which of the following is the most appropriate pharmacotherapy?
A 43-year-old man with HIV infection comes to the physician because of a 2-week history of progressive diarrhea and a 3-kg (6.6-lb) weight loss. During this period, he has had 3–4 episodes of watery stools daily, with multiple instances of blood in the stool. He is currently receiving antiretroviral therapy with zidovudine, lamivudine, and dolutegravir. Physical examination shows pallor and dry mucous membranes. A colonoscopy shows multiple linear ulcers. Polymerase chain reaction of a stool sample is positive for cytomegalovirus. Treatment with valganciclovir is begun. Adding this drug to his current medication regimen puts this patient at greatest risk for which of the following adverse effects?
A 59-year-old woman comes to the physician for a routine health maintenance examination. She feels well. She has systemic lupus erythematosus and hypertension. She does not drink alcohol. Her current medications include lisinopril and hydroxychloroquine. She appears malnourished. Her vital signs are within normal limits. Examination shows a soft, nontender abdomen. There is no ascites or hepatosplenomegaly. Serum studies show: Total bilirubin 1.2 mg/dL Alkaline phosphatase 60 U/L Alanine aminotransferase 456 U/L Aspartate aminotransferase 145 U/L Hepatitis A IgM antibody negative Hepatitis A IgG antibody positive Hepatitis B surface antigen positive Hepatitis B surface antibody negative Hepatitis B envelope antigen positive Hepatitis B envelope antibody negative Hepatitis B core antigen IgM antibody negative Hepatitis B core antigen IgG antibody positive Hepatitis C antibody negative Which of the following is the most appropriate treatment for this patient?
A 44-year-old man comes to the physician for a follow-up examination. Eight months ago, he was diagnosed with HIV infection and combined antiretroviral treatment was begun. He feels well. He does not smoke or drink alcohol. Current medications include lamivudine, zidovudine, atazanavir, and trimethoprim-sulfamethoxazole. Laboratory studies show: Hemoglobin 11.2 g/dL Mean corpuscular volume 102 μm3 Leukocyte count 2,600/mm3 Segmented neutrophils 38% Lymphocytes 54% Platelet count 150,000/mm3 Serum Folate normal Lactate 6.0 mEq/L (N = 0.5–2.2) Arterial blood gas analysis on room air shows: pH 7.34 pCO2 55 mm Hg pO2 99 mmHg HCO3- 14 mEq/L The drug most likely responsible for this patient's current laboratory findings belongs to which of the following classes of drugs?
A 26-year-old female medical student presents to occupational health after sustaining a needlestick injury. She reports that she was drawing blood from an HIV-positive patient when she stuck herself percutaneously while capping the needle. She immediately washed the puncture wound with betadine. The medical student has a negative HIV serology from the beginning of medical school two years ago. She is monogamous with one male partner and denies any intravenous drug use. The source patient was recently diagnosed with HIV, and has a CD4 count of 550 cells/µL. His most recent viral load is 1,800,000 copies/mL, and he was started on HAART three days ago. Which of the following is the best next step to manage the female medical student’s exposure?
Practice by Chapter
HIV protease inhibitors
Practice Questions
HIV reverse transcriptase inhibitors
Practice Questions
HIV integrase inhibitors
Practice Questions
HIV entry inhibitors
Practice Questions
Hepatitis B antivirals
Practice Questions
Hepatitis C direct-acting antivirals
Practice Questions
Influenza antivirals
Practice Questions
Herpesvirus antivirals
Practice Questions
Cytomegalovirus antivirals
Practice Questions
Respiratory syncytial virus therapies
Practice Questions
Broad-spectrum antivirals
Practice Questions
Antiretroviral resistance
Practice Questions
Antiviral prophylaxis strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app