
Antimicrobials — MCQs

On this page
A 4-year-old girl is brought to the emergency department by her father for the evaluation of abdominal pain for 1 hour after drinking a bottle of rust remover. The father reports that she vomited once on the way to the hospital and that her vomit was not bloody. The patient has pain with swallowing. She appears uncomfortable. Oral examination shows mild erythema of the epiglottis and heavy salivation. Which of the following is the most likely long-term complication in this patient?
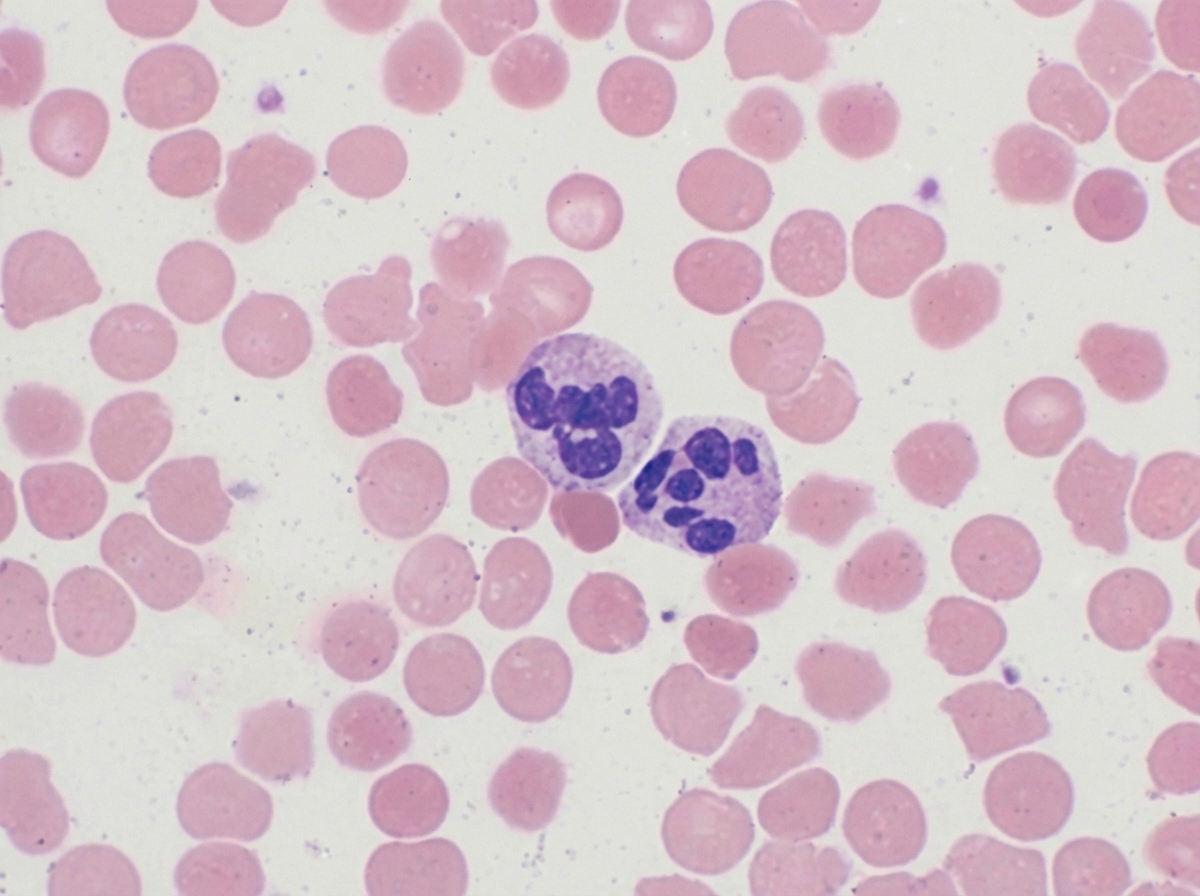
A 52-year-old female presents to her rheumatologist with complaints of fatigue, a sore mouth, and occasional nausea and abdominal pain over the past several months. Her medical history is significant for 'pre-diabetes' treated with diet and exercise, hypertension managed with lisinopril, and rheumatoid arthritis well-controlled with methotrexate. Her vital signs are within normal limits. Physical examination is significant for an overweight female with oral ulcerations and glossitis. The physician orders laboratory work-up including complete blood count with peripheral blood smear as well as basic metabolic panel and serum methylmalonic acid and homocysteine levels. These tests are significant for a hematocrit of 29.5, a decreased reticulocyte count, normal serum methylmalonic acid level, increased homocysteine level, as well as the peripheral smear shown in Figure C. Which of the following could have reduced this patient's risk of developing their presenting condition?
A 7-month-old girl is brought to the pediatrician by her parents with a mild, persistent fever for the past week. The patient’s mother also states she is feeding poorly and has become somewhat lethargic. The patient was born at term and the delivery was uncomplicated. The child’s birth weight was 3.5 kg (7.7 lb) and at 6 months was 7.0 kg (15.4 lb). She is fully immunized. The patient’s father recently returned from a business trip to India with a mild cough and was diagnosed with tuberculosis. The patient’s mother tests negative for tuberculosis The patient’s temperature is 38.1℃ (100.5℉). Today, she weighs 7.0 kg (15.4 lb). Cardiopulmonary auscultation reveals diminished breath sounds in the upper lobes. A chest radiograph demonstrates hilar lymphadenopathy and infiltrates in the upper lobes. Gastric aspirates are positive for acid-fast bacilli, however, cultures are still pending. Father and daughter are both started on standard antitubercular therapy. Which of the following is the appropriate management for the patient’s mother?
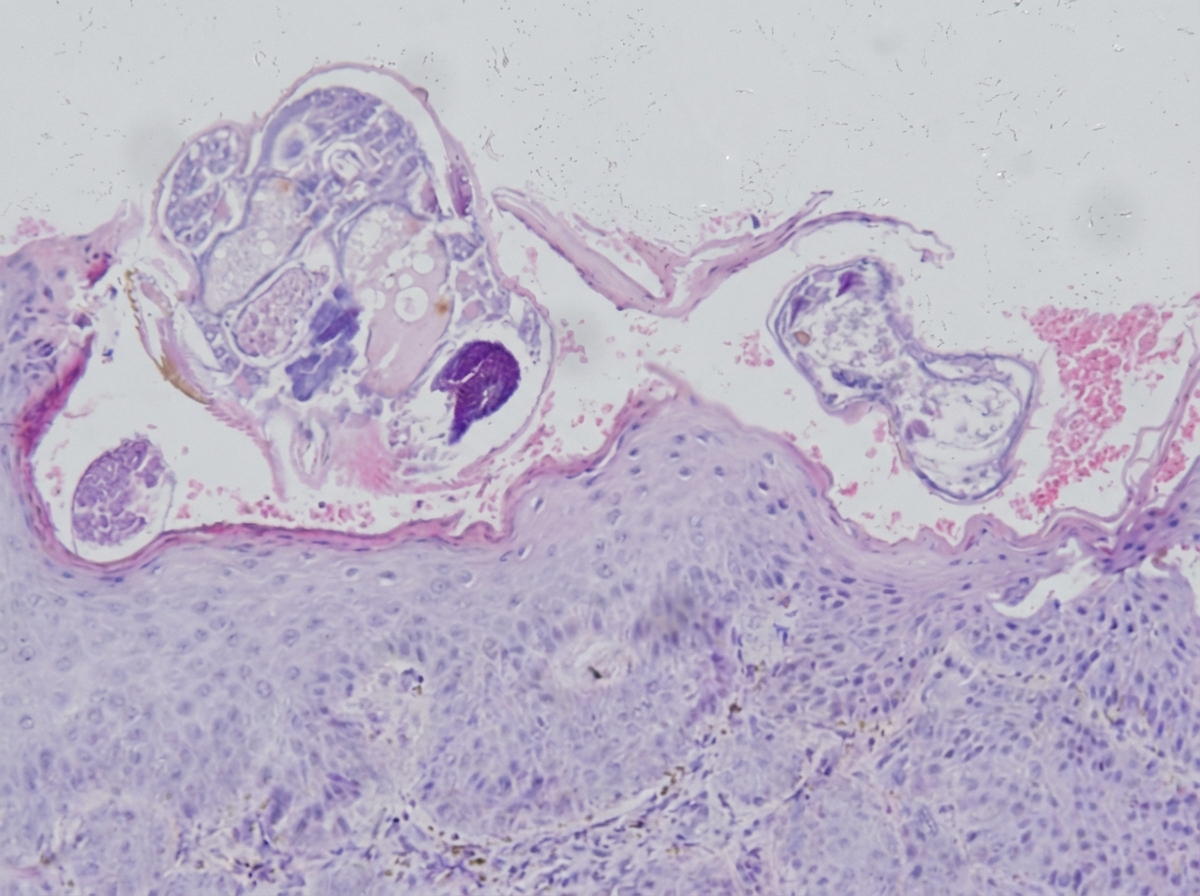
A 37-year-old woman with a history of systemic lupus erythematosus, on prednisone and methotrexate, presents to the dermatology clinic with three weeks of a diffuse, itchy rash. Physical exam is remarkable for small red papules in her bilateral axillae and groin and thin reddish-brown lines in her interdigital spaces. The following skin biopsy is obtained. Which of the following is the most appropriate treatment?
A 42-year-old man with non-small cell lung cancer is enrolled in a clinical trial for a new chemotherapeutic drug. The drug prevents microtubule depolymerization by binding to the beta subunit of tubulin. The mechanism of action of this new drug is most similar to which of the following?
A 33-year-old Hispanic woman who recently immigrated to the United States with her newborn daughter is presenting to a free clinic for a wellness checkup for her baby. As part of screening for those immigrating or seeking refuge in the United States, she and her child are both evaluated for tuberculosis. The child’s purified protein derivative (PPD) test and chest radiograph are negative, and although the mother’s chest radiograph is also negative, her PPD is positive. She states that she is currently asymptomatic and has no known history of tuberculosis (TB). The mother’s vital signs include: blood pressure 124/76 mm Hg, heart rate 74/min, and respiratory rate 14/min. She is advised to begin treatment with isoniazid, supplemented with pyridoxine for the next 9 months. She asks about the potential for harm to the child if she begins this course of treatment since she is breastfeeding. Which of the following is the most appropriate response to this patient’s concerns?
A 54-year-old woman presents with acute pain in her left toe. She says she hasn't been able to wear closed shoes for 2 weeks. Past medical history is significant for gastroesophageal reflux disease, diagnosed 2 years ago. The patient is afebrile and vital signs are within normal limits. Her BMI is 31 kg/m2. On physical examination, the left toe is warm to touch, swollen, and erythematous. A joint fluid aspiration from the left toe is performed and shows needle-shaped negatively birefringent urate crystals. The patient is started on methotrexate for gout prophylaxis. On her follow-up visit 6 weeks later, she has an elevated homocysteine level, a decreased serum folic acid level, and a normal methylmalonic acid level. Which of the following drugs would most likely cause a similar side effect to that seen in this patient?
A 22-year-old female with a history of bipolar disease presents to the emergency room following an attempted suicide. She reports that she swallowed a bottle of pain reliever pills she found in the medicine cabinet five hours ago. She currently reports malaise, nausea, and anorexia. She has vomited several times. Her history is also notable for alcohol abuse. Her temperature is 99.4°F (37.4°C), blood pressure is 140/90 mmHg, pulse is 90/min, and respirations are 20/min. Physical examination reveals a pale, diaphoretic female in distress with mild right upper quadrant tenderness to palpation. Liver function tests and coagulation studies are shown below: Serum: Alkaline phosphatase: 110 U/L Aspartate aminotransferase (AST, GOT): 612 U/L Alanine aminotransferase (ALT, GPT): 557 U/L Bilirubin, Total: 2.7 mg/dl Bilirubin, Direct: 1.5 mg/dl Prothrombin time: 21.7 seconds Partial thromboplastin time (activated): 31 seconds International normalized ratio: 2.0 Serum and urine drug levels are pending. Which of the following medications should be administered to this patient?
A 67-year-old woman presents to the infectious disease clinic after her PPD was found to be positive. A subsequent chest radiography shows a cavity in the apex of the right upper lobe, along with significant hilar adenopathy. The patient is diagnosed with tuberculosis and is started on the standard four-drug treatment regimen. Four weeks later, she returns for her first follow-up appointment in panic because her eyes have taken on an orange/red hue. Which of the following describes the mechanism of action of the drug most likely responsible for this side effect?
A 60-year-old man comes to the physician because of persistent fatigue over the past ten months. His previous annual health maintenance examination showed no abnormalities. He appears pale. Physical examination shows numerous petechial lesions over the abdomen and marked splenomegaly. His serum hemoglobin concentration is 9.4 g/dL, leukocyte count is 4,100/mm3, and thrombocyte count is 110,000/mm3. A peripheral blood smear shows large white blood cells with centrally placed nuclei and multiple fine, radial cytoplasmic projections that stain positively for tartrate-resistant acid phosphatase (TRAP). Which of the following is the most likely characteristic of the medication used as first-line treatment for this patient's condition?
Practice by Chapter
Antiparasitic drugs (antiprotozoals)
Practice Questions
Antimalarial medications
Practice Questions
Anthelmintics
Practice Questions
Antiseptics and disinfectants
Practice Questions
Antimicrobial stewardship principles
Practice Questions
Empiric antimicrobial selection
Practice Questions
Antimicrobial dosing in special populations
Practice Questions
Antimicrobial pharmacokinetics/pharmacodynamics
Practice Questions
Antimicrobial toxicities
Practice Questions
Antimicrobial allergies and cross-reactivity
Practice Questions
Combination antimicrobial therapy
Practice Questions
Cost-effective antimicrobial strategies
Practice Questions
New antimicrobial development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app