
Antimicrobials — MCQs

On this page
A 25-year-old man presents to the physician with 2 days of profuse, watery diarrhea. He denies seeing blood or mucus in the stools. On further questioning, he reveals that he eats a well-balanced diet and generally prepares his meals at home. He remembers having some shellfish from a street vendor 3 days ago. He takes no medications. His past medical history is unremarkable. Which of the following mechanisms most likely accounts for this patient’s illness?
A researcher is studying a new antituberculosis drug. In the laboratory, the drug has been shown to be effective against mycobacteria located within phagolysosomes of macrophages, but it is also significantly less effective against extracellular tuberculoid bacteria. The characteristics of this drug are most similar to which of the following agents?
A 44-year-old woman presents to the emergency department with a headache, vertigo, confusion, and dyspnea. A relevant history cannot be obtained from the patient because she seems confused and gives incoherent responses to questions. Her husband says that she was cleaning the kitchen this morning until the curtains caught on fire earlier this morning from the stove’s flame. Her vitals include: pulse 100/min, respirations 20/min, blood pressure 130/80 mm Hg, oxygen saturation 97% on room air. On physical examination, the patient is oriented x 0. The skin has a bright cherry-red color. Laboratory testing shows: pH 7.35 PaO2 90 mm Hg pCO2 40 mm Hg HCO3- 26 mEq/L SpO2 97% Blood lactate 11 mmol/L Which of the following is the most likely diagnosis in this patient?
A 28-year-old woman comes to the physician because of a two-month history of fatigue and low-grade fevers. Over the past 4 weeks, she has had increasing shortness of breath, a productive cough, and a 5.4-kg (11.9-lb) weight loss. Three months ago, the patient returned from a two-month trip to China. The patient appears thin. Her temperature is 37.9°C (100.2°F), pulse is 75/min, and blood pressure is 125/70 mm Hg. Examination shows lymphadenopathy of the anterior and posterior cervical chain. Rales are heard at the left lower lobe of the lung on auscultation. Laboratory studies show a leukocyte count of 11,300/mm3 and an erythrocyte sedimentation rate of 90 mm/h. An x-ray of the chest shows a patchy infiltrate in the left lower lobe and ipsilateral hilar enlargement. Microscopic examination of the sputum reveals acid-fast bacilli; polymerase chain reaction is positive. Sputum cultures are pending. After placing the patient in an airborne infection isolation room, which of the following is the most appropriate next step in management?
A 13-year-old girl presents with a 4-week history of unrelenting cough, night sweats, and fever. No known past medical history and no current medications. The patient recently immigrated to the country from a rural town in northern India. Vaccination status is unknown. Her temperature is 38.5°C (101.3°F), pulse is 115/min, blood pressure is 95/65 mm Hg, and respiratory rate is 22/min. Physical examination is significant for decreased breath sounds in the right upper lobe and multiple right cervical lymphadenopathies. A chest radiograph reveals multiple cavitations in the right upper lobe and right hilar lymphadenopathy. A sputum culture shows acid-fast bacilli. Which of the following compounds must be included in addition to the recommended antimicrobial therapy in this patient?
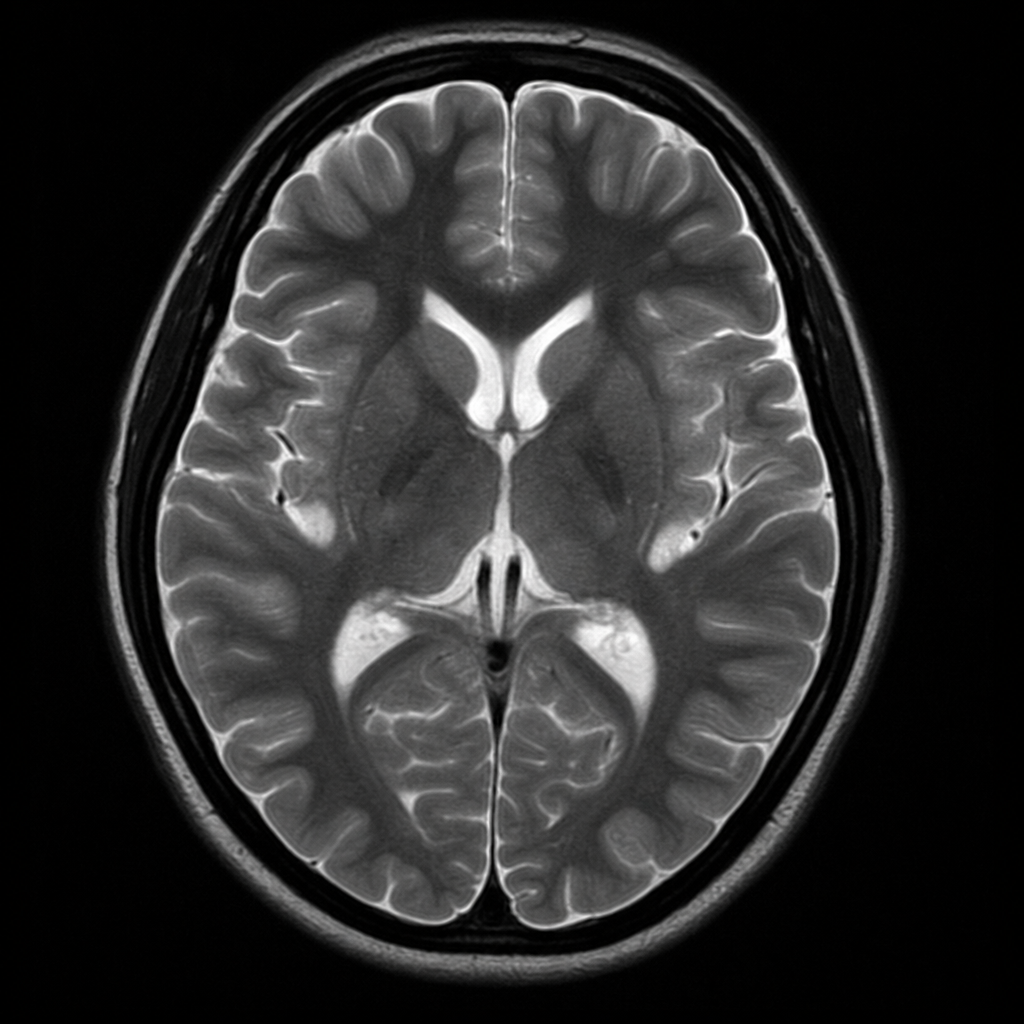
A 29-year-old man from India seeks evaluation at a clinic with complaints of sore muscles and lethargy of several days duration. After the physical examination and laboratory testing, the patient is asked to stay for treatment and monitoring. Despite the physician's warning, the patient leaves the hospital against medical advice. He subsequently develops difficulty in breathing and anuria and is brought to the emergency department with loss of consciousness. The patient gets an immediate T2 weighted image of his head, which is shown in the exhibit. Laboratory findings confirm the presence of rings, which appear on the periphery of red blood cells (RBCs). What is the best treatment for his condition?
A 78-year-old man receives chemotherapy for advanced hepatocellular carcinoma. Despite appropriate therapy, he dies 4 months later. Histopathological examination of the cancer cells shows the presence of a transmembrane efflux pump protein that is known to cause decreased intracellular concentrations of chemotherapeutic drugs. Which of the following best describes this membrane protein?
A 33-year-old woman comes to the physician for a routine health maintenance examination. She feels well. She was diagnosed with multiple sclerosis one year ago. She has had two exacerbations since then, each lasting about one week and each requiring hospitalization for corticosteroid treatment. Her most recent exacerbation was three weeks ago. In between these episodes she has had no neurologic symptoms. She takes a multivitamin and a calcium supplement daily. Her vital signs are within normal limits. Examination, including neurologic examination, shows no abnormalities. Which of the following is the most appropriate next step in pharmacotherapy?
A 44-year-old man, with a history of intravenous (IV) drug use, presented to the emergency department due to worsening non-productive cough, exertional dyspnea, and night sweats. His cough started 3 weeks ago and progressively worsened. He is homeless and well-known by the hospital staff. He was previously admitted to the hospital after an overdose of opioids. He takes no medication. At the hospital, the vital signs included: blood pressure 101/68 mm Hg, heart rate 99/min, respiratory rate 20/min, oxygen saturation of 91% on room air, and oral temperature of 37.4°C (99.3°F). His chest X-ray showed left perihilar shadowing. The laboratory results included: WBC count 8,800/mm3 Arterial pH 7.39 Rapid HIV testing positive with an elevated viral load PaCO2 41 mm Hg PaO2 76 mm Hg He was admitted for the treatment of presumed sepsis and pneumonia, and he was immediately started on IV ceftriaxone. An induced sputum specimen shows multiple kidney bean-shaped cysts that are approximately 5 um. These cysts stain positive with methenamine silver. What is the preferred antibiotic therapeutic regimen for this condition?
A 15-year-old boy comes to the physician because of skin changes on his face, chest, and back over the past year. Treatment with over-the-counter benzoyl peroxide has been ineffective. Physical examination shows numerous open comedones, inflammatory papules, and pustules on his face, chest, and back. Which of the following is the most likely underlying mechanism of this patient’s skin condition?
Practice by Chapter
Antiparasitic drugs (antiprotozoals)
Practice Questions
Antimalarial medications
Practice Questions
Anthelmintics
Practice Questions
Antiseptics and disinfectants
Practice Questions
Antimicrobial stewardship principles
Practice Questions
Empiric antimicrobial selection
Practice Questions
Antimicrobial dosing in special populations
Practice Questions
Antimicrobial pharmacokinetics/pharmacodynamics
Practice Questions
Antimicrobial toxicities
Practice Questions
Antimicrobial allergies and cross-reactivity
Practice Questions
Combination antimicrobial therapy
Practice Questions
Cost-effective antimicrobial strategies
Practice Questions
New antimicrobial development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app