
Antimicrobials — MCQs

On this page
A 67-year-old male with a past medical history of diabetes type II, obesity, and hyperlipidemia presents to the general medical clinic with bilateral hearing loss. He also reports new onset vertigo and ataxia. The symptoms started a day after undergoing an uncomplicated cholecystectomy. If a drug given prophylactically just prior to surgery has caused this patient’s symptoms, what is the mechanism of action of the drug?
A 70-year-old woman presents with numbness and tingling that is worse in the soles of her feet. She says that symptoms started a few weeks ago and have progressively worsened. She also complains of mild nausea and white lines on her fingernails. Past medical history is significant for diabetes mellitus type 2, managed with metformin. Her last HbA1c was 5.8%. The patient denies any changes in her vision, chest pain, or palpitations. She says she lives near an industrial area that was in the newspaper for leaking waste into the groundwater but she can’t remember the details. She also says she spends a lot of her free time in her garden. On physical examination, there is decreased fine touch, temperature, and vibrational sensation in the extremities bilaterally Strength is reduced symmetrically 4 out of 5 in all limbs along with reduced (1+) deep tendon reflexes. Which of the following is the best treatment option for this patient?
A 22-year-old woman comes to the physician because of abdominal pain and diarrhea for 2 months. The pain is intermittent, colicky and localized to her right lower quadrant. She has anorexia and fears eating due to the pain. She has lost 4 kg (8.8 lb) during this time. She has no history of a serious illness and takes no medications. Her temperature is 37.8°C (100.0°F), blood pressure 125/65 mm Hg, pulse 75/min, and respirations 14/min. An abdominal examination shows mild tenderness of the right lower quadrant on deep palpation without guarding. Colonoscopy shows small aphthous-like ulcers in the right colon and terminal ileum. Biopsy from the terminal ileum shows noncaseating granulomas in all layers of the bowel wall. Which of the following is the most appropriate pharmacotherapy at this time?
A research group wants to assess the safety and toxicity profile of a new drug. A clinical trial is conducted with 20 volunteers to estimate the maximum tolerated dose and monitor the apparent toxicity of the drug. The study design is best described as which of the following phases of a clinical trial?
A 3-year-old boy is brought to his pediatrician by his mother when he developed redness, burning, itching, and exquisite pain all over his arms, lower legs, neck, and face. The mother states that she just recently began taking him to the local playground in the afternoons. She reports that she applied liberal amounts of sunscreen before and during the time outside. She states that they were at the playground for 30 minutes to 1 hour each day for the last 3 days. The patient has experienced prior episodes of redness and pain after being outdoors, but they were relatively minor and resolved within 12 hours. She says his current presentation is much more severe with more exquisite pain than in the past. The patient's vital signs are as follows: T 37.2 C, HR 98, BP 110/62, RR 16, and SpO2 99%. Physical examination reveals edema, erythema, and petechiae over the patient's face, neck, arms, and lower legs. No blistering or scarring of the skin is noted. Which of the following is the best treatment option for this patient's condition?
A 36-year-old woman comes to the physician because of prolonged stiffness in the morning and progressive pain and swelling of her wrists and hands over the past 4 months. Examination shows bilateral swelling and mild tenderness of the wrists and the second, third, and fourth metacarpophalangeal joints. Her range of motion is limited by pain. Serum studies show elevated anti-cyclic citrullinated peptide antibodies. Treatment with methotrexate is begun. At a follow-up examination, her serum aspartate aminotransferase (AST) concentration is 75 U/L and her serum alanine aminotransferase (ALT) concentration is 81 U/L. Which of the following substances is essential for the function of these enzymes?
A 45-year-old homeless man presents to the emergency department with a 1-week history of an intensely pruritic, red rash on his hands, wrists, and finger webs. The itching is worse at night. Physical examination reveals small, erythematous papules and burrows. A topical drug with which of the following mechanisms of action is most likely to be effective in treating this condition?
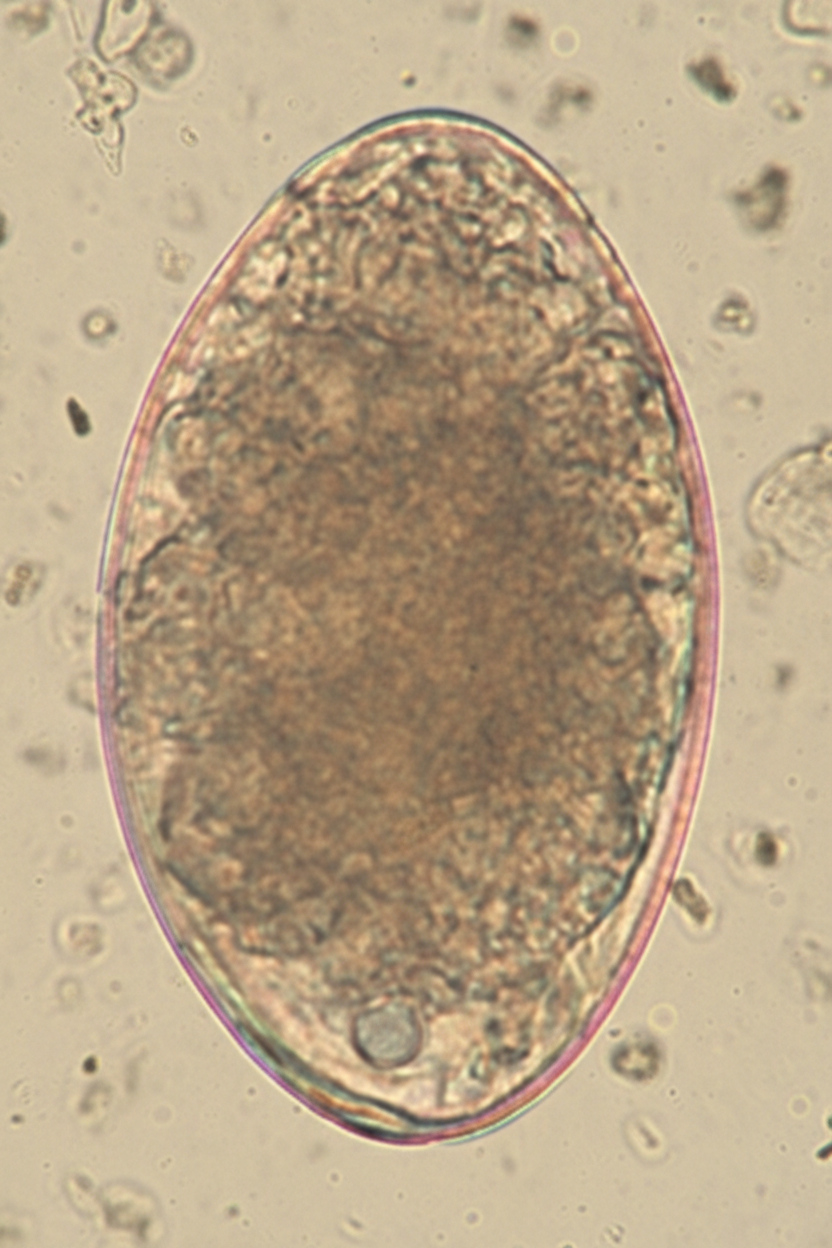
A 7-year-old girl is brought to the physician by her mother because of a 4-week history of irritability, diarrhea, and a 2.2-kg (5-lb) weight loss that was preceded by a dry cough. The family returned from a vacation to Indonesia 2 months ago. Her vital signs are within normal limits. Abdominal examination shows mild tenderness with no guarding or rebound and increased bowel sounds. Her leukocyte count is 9,200/mm3 with 20% eosinophils. A photomicrograph of a wet stool mount is shown. Which of the following is the most appropriate pharmacotherapy?
An 8-year-old boy is brought to the physician because of a 1-day history of severe left hand pain. He has had similar painful episodes in the past that required hospitalization. Physical examination shows pale conjunctivae. There is tenderness on palpation of the wrist and the small joints of the left hand. Peripheral blood smear shows crescent-shaped erythrocytes. He is started on a pharmacologic agent that is known to cause macrocytosis. This drug causes an arrest in which of the following cell cycle phases?
A 33-year-old woman presents to her local clinic in rural eastern India complaining of neck pain and fever. She reports a 4 day history of severe neck pain, neck stiffness, mild diarrhea, and fever. She has not taken her temperature. She works as a laborer and frequently carries heavy weights on her back. She is prescribed a medication and told to come back if her symptoms do not improve. Her symptoms resolve after a couple days. Six months later, she gives birth to a newborn male at 34 weeks gestation. His temperature is 97.8°F (36.6°C), blood pressure is 90/55 mmHg, pulse is 110/min, and respirations are 24/min. On examination, the baby is irritable with a weak cry. Ashen gray cyanosis is noted diffusely. What is the mechanism of action of the drug responsible for this child's presentation?
Practice by Chapter
Antiparasitic drugs (antiprotozoals)
Practice Questions
Antimalarial medications
Practice Questions
Anthelmintics
Practice Questions
Antiseptics and disinfectants
Practice Questions
Antimicrobial stewardship principles
Practice Questions
Empiric antimicrobial selection
Practice Questions
Antimicrobial dosing in special populations
Practice Questions
Antimicrobial pharmacokinetics/pharmacodynamics
Practice Questions
Antimicrobial toxicities
Practice Questions
Antimicrobial allergies and cross-reactivity
Practice Questions
Combination antimicrobial therapy
Practice Questions
Cost-effective antimicrobial strategies
Practice Questions
New antimicrobial development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app