
Antimicrobials — MCQs

On this page
A 49-year-old man presents with an 11-month history of progressive fatigue. He denies any night sweats, weight loss, abdominal pain, nausea, vomiting, change in bowel habits, or bleeding. He has no significant past medical history. His vital signs include: temperature 37.0°C (98.6°F), blood pressure 119/81 mm Hg, pulse 83/min, and respiratory rate 19/min. On physical examination, mild splenomegaly is noted on abdominal percussion. Laboratory findings are significant for a leukocyte count of 16,700/mm3 and a low serum leukocyte alkaline phosphatase (LAP) score. A bone marrow biopsy is performed, which shows marked hypercellularity with a clear dominance of granulocytes. Cytogenetic analysis is positive for the Ph1 gene. Which of the following is the best course of treatment for this patient?
A 20-year-old college student is brought to the ED after a motor vehicle accident. Primary and secondary surveys reveal no significant compromise to his airway, his cardiovascular system, or to his motor function. However, his conjunctiva appear injected and he maintains combative behavior towards staff. What is the gold standard confirmatory test for substance use?
A hospitalized 45-year-old man has had mild flank pain since awakening 3 hours ago. He also reports a new generalized rash. Two weeks ago, he was diagnosed with pulmonary tuberculosis. Current medications include isoniazid, pyrazinamide, rifampin, ethambutol, and pyridoxine. His temperature is 38.3°C (100.9°F), pulse is 74/min, and blood pressure is 128/72 mm Hg. Examination of the skin shows diffuse erythema with confluent papules. There is no costovertebral angle tenderness. Laboratory studies show: Leukocyte count 9,800/mm3 Segmented neutrophils 59% Bands 3% Eosinophils 4% Lymphocytes 29% Monocytes 5% Serum Urea nitrogen 25 mg/dL Creatinine 1.9 mg/dL Urine WBC 8–10/hpf Eosinophils numerous RBC 5–6/hpf RBC casts negative WBC casts numerous In addition to intravenous fluid resuscitation, which of the following is the most appropriate next step in management?
A 36-year-old male with fluctuating levels of consciousness is brought to the emergency department by ambulance due to a fire in his home. He currently opens his eyes to voice, localizes painful stimuli, responds when asked questions, but is disoriented and cannot obey commands. The patient’s temperature is 99°F (37.2°C), blood pressure is 86/52 mmHg, pulse is 88/min, and respirations are 14/min with an oxygen saturation of 97% O2 on room air. Physical exam shows evidence of soot around the patient’s nose and mouth, but no burns, airway obstruction, nor accessory muscle use. A blood lactate is 14 mmol/L. The patient is started on intravenous fluids. What is the next best step in management?
A 62-year-old woman presents with abdominal pain and blood in her urine. Since the acute onset of symptoms 3 days ago, there has been no improvement. She describes the pain as moderate, sharp and burning in character, non-radiating, and localized to the suprapubic region. She also has noted some mild urinary frequency and urgency for the past 5 days, which has been getting progressively worse. She denies any flank pain, fever, chills, night sweats, dysuria, or pain on urination. The patient has a history of an abdominal leiomyosarcoma, which was diagnosed 6 months ago. The course of her disease is complicated by hepatic metastases, for which she recently started receiving a new therapy. The patient reports a 15-pack-year smoking history, but no alcohol or recreational drug use. Her temperature is 37.0℃ (98.6℉), pulse is 84/min, respiratory rate is 18/min, and blood pressure is 110/75 mm Hg. On physical examination, there is some mild suprapubic tenderness to palpation. The remainder of the exam is unremarkable. Laboratory findings include a mild leukopenia of 3,000/mm3. A urine dipstick reveals 3+ blood. Which of the following best describes the medication that could have prevented this patient’s symptoms?
A 38-year-old woman presents to her primary care physician for a new patient appointment. She states that she feels well and has no current complaints. The patient recently started seeing a specialist for treatment for another medical condition but otherwise has had no medical problems. The patient lives alone and drinks 2 alcoholic beverages every night. She has had 3 sexual partners in her lifetime, uses oral contraceptive pills for contraception, and has never been pregnant. Physical exam reveals a pleasant, obese woman with normal S1 and S2 on cardiac exam. Musculoskeletal exam reveals swelling of the MCP and PIP joints of the hands as well as ulnar deviation of the fingers. Laboratory tests are ordered and results are below: Serum: Na+: 139 mEq/L Cl-: 100 mEq/L K+: 4.3 mEq/L HCO3-: 25 mEq/L BUN: 20 mg/dL Glucose: 99 mg/dL Creatinine: 1.1 mg/dL Ca2+: 10.2 mg/dL AST: 95 U/L ALT: 68 U/L Which of the following best explains this patient's abnormal laboratory values?
A 67-year-old man comes to the physician for a follow-up examination after he was diagnosed with mantle cell lymphoma. The physician recommends a chemotherapeutic regimen containing bortezomib. Which of the following best describes the effect of this drug?
A 55-year-old man with a history of fatigue and exertional dyspnea presents to the urgent care clinic following an acute upper respiratory illness. On physical examination, his pulses are bounding, his complexion is very pale, and scleral icterus is apparent. The spleen is moderately enlarged. Oxygen saturation is 79% at rest, with a new oxygen requirement of 9 L by a non-rebreather mask. Laboratory analysis results show a hemoglobin level of 6.8 g/dL. Of the following options, which hypersensitivity reaction does this condition represent?
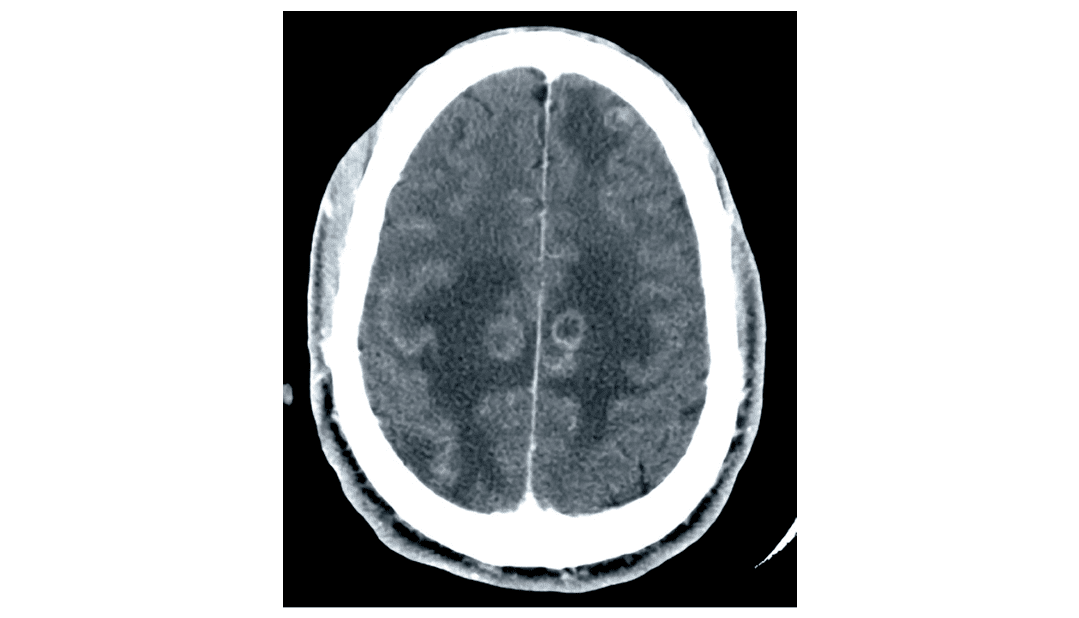
A 35-year-old man is brought to the emergency department after experiencing a seizure. According to his girlfriend, he has had fatigue for the last 3 days and became confused this morning, after which he started having uncontrollable convulsions throughout his entire body. He was unconscious throughout the episode, which lasted about 4 minutes. He has not visited a physician for over 10 years. He has smoked one pack of cigarettes daily for 12 years. His girlfriend admits they occasionally use heroin together with their friends. His temperature is 38.8°C (101.8°F), pulse is 93/min, respirations are 20/min, and blood pressure is 110/70 mm Hg. The lungs are clear to auscultation and examination shows normal heart sounds and no carotid or femoral bruits. He appears emaciated and somnolent. There are multiple track marks on both his arms. He is unable to cooperate for a neurological exam. Laboratory studies show a leukocyte count of 3,000/mm3, a hematocrit of 34%, a platelet count of 354,000/mm3, and an erythrocyte sedimentation rate of 27 mm/h. His CD4+ T-lymphocyte count is 84/mm3 (normal ≥ 500). A CT scan of the head is shown. Which of the following is the most appropriate next step considering this patient's CT scan findings?
A 56-year-old man of Nepalese origin presents to a clinic complaining of skin rashes that have been troubling him for years. On examination, there are numerous poorly demarcated skin lesions present on all parts of the body. There is also evidence of significant facial thickening, eyebrow loss, and symmetrical sensory neuropathy in a ‘glove and stocking’ distribution. An examination of the hands reveals bilateral weakness. A skin biopsy is taken from one of the lesions, and the culture is positive for acid-fast bacilli. Which of the following pharmacological therapies is involved in the treatment of this condition?
Practice by Chapter
Antiparasitic drugs (antiprotozoals)
Practice Questions
Antimalarial medications
Practice Questions
Anthelmintics
Practice Questions
Antiseptics and disinfectants
Practice Questions
Antimicrobial stewardship principles
Practice Questions
Empiric antimicrobial selection
Practice Questions
Antimicrobial dosing in special populations
Practice Questions
Antimicrobial pharmacokinetics/pharmacodynamics
Practice Questions
Antimicrobial toxicities
Practice Questions
Antimicrobial allergies and cross-reactivity
Practice Questions
Combination antimicrobial therapy
Practice Questions
Cost-effective antimicrobial strategies
Practice Questions
New antimicrobial development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app