
Antimicrobials — MCQs

On this page
A 48-year-old woman presented to the hospital with a headache, intermittent fevers and chills, generalized arthralgias, excessive thirst, increased fluid intake, and a progressive rash that developed on her back. Three days before seeking evaluation at the hospital, she noticed a small, slightly raised lesion appearing like a spider or insect bite on her back, which she considered to be a scab covering the affected region. The patient's fever reached 39.4°C (102.9°F) 2 days before coming to the hospital, with an intensifying burning sensation on the affected site. When a family member examined the bite, it was noticed that the bump had transformed into a circular rash. The patient took over-the-counter ibuprofen for intense pain so she could sleep through the night. The day before her hospital visit, the patient felt exhausted but managed to complete a normal workday. On the day of the hospital visit, she awoke feeling very ill, with shooting joint pains, high fevers, and excessive thirst, which led to her to seek medical attention. On physical examination, her temperature was 40.1°C (104.2°F), and there was a large circular red rash with a bulls-eye appearance (17 × 19 cm in diameter) on her back. The rest of the physical examination was unremarkable. Her past medical and surgical histories were not significant apart from a history of anaphylaxis when taking a tetracycline. She recalled a walk in the woods 3 weeks before this exam but denied finding a tick or any other ectoparasite on her body. She denied any nutritional or inhalational allergies, although she emphasized that she is allergic to tetracyclines. Based on her symptoms, medical history, and physical examination findings, the attending physician decides to institute antimicrobial therapy immediately. Which antimicrobial drug did the physician prescribe?
A 25-year-old man comes to the physician because of diarrhea, bloating, nausea, and vomiting for the past 3 days. He describes his stool as soft, frothy, and greasy. He denies seeing blood in stool. The patient went on a hiking trip last week and drank fresh water from the stream. Three months ago, he was on vacation with his family for 2 weeks in Brazil, where he tried many traditional dishes. He also had watery diarrhea and stomach cramping for 3 days during his visit there. He has no history of serious illness. He takes no medications. The patient appears dehydrated. His temperature is 37°C (98.6°F), blood pressure is 100/60 mm Hg, pulse is 80/min, and respirations are 12/min. Examination shows dry mucous membranes and diffuse abdominal tenderness. Microscopy of the stool reveals cysts. Which of the following is the most appropriate next step in management?
A 60-year-old man presents to the emergency department with shortness of breath, cough, and fever. He states that his symptoms started a few days ago and have been progressively worsening. The patient recently returned from international travel. He works from home and manages a chicken coop as a hobby. He has a past medical history of an ST-elevation myocardial infarction and recently has had multiple sick contacts. His temperature is 102°F (38.9°C), blood pressure is 187/108 mmHg, pulse is 120/min, respirations are 17/min, and oxygen saturation is 93% on room air. A radiograph of the chest reveals bilateral pleural effusions. Pleurocentesis demonstrates the findings below: Protein ratio (pleural/serum): 0.8 Lactate dehydrogenase ratio (pleural/serum): 0.75 Glucose: 25 mg/dL Further analysis reveals a lymphocytic leukocytosis of the pleural fluid. Which of the following is the next best step in management?
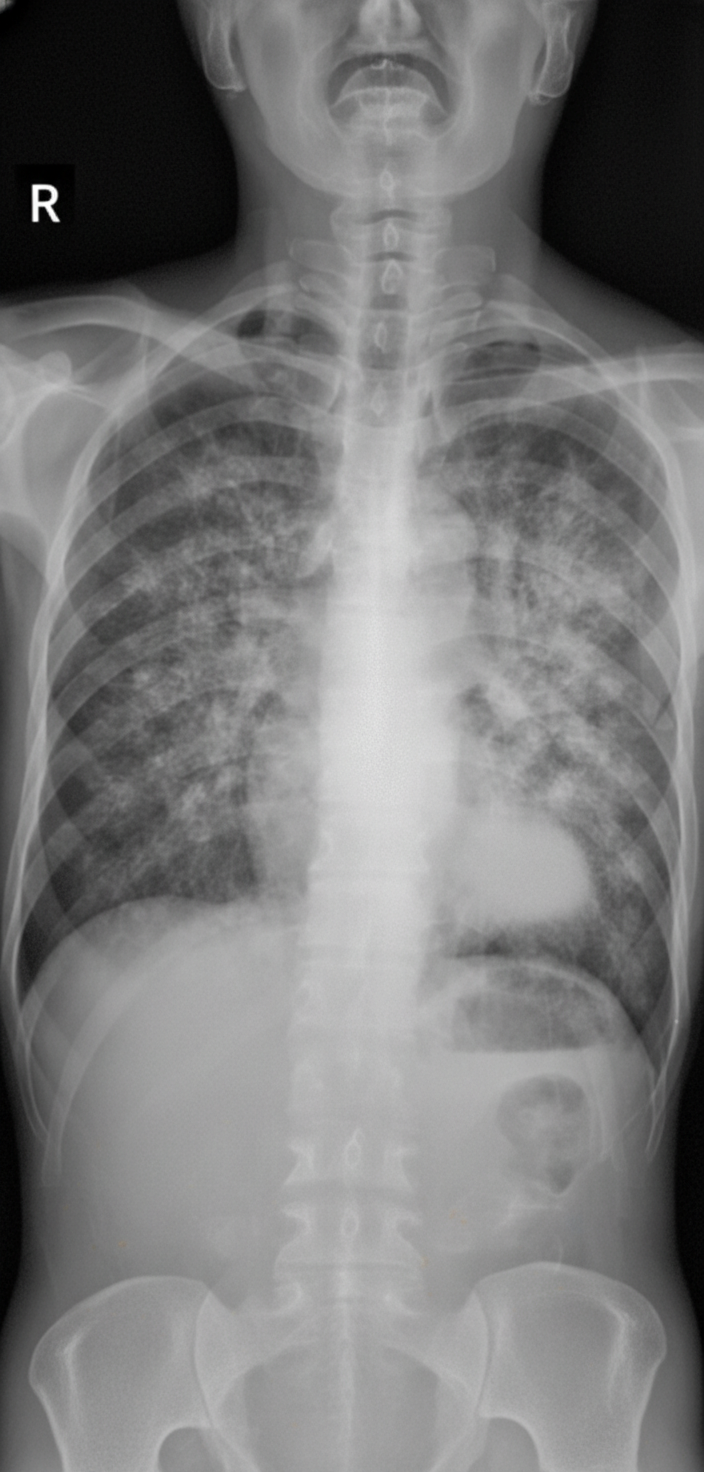
A 67-year-old male with HIV (not on antiretroviral therapy, CD4 count 85 cells/µL) presents to the emergency room with dry cough and malaise. He has no other complaints. His vital signs are T 100.4 F (38 C), O2 93% on room air, RR 20, BP 115/75 mmHg. Physical examination is notable for crackles bilaterally. A chest radiograph is obtained (Image A). The patient is admitted and initially treated with guideline-compliant antibiotics for community-acquired pneumonia. Unfortunately, his respiratory function deteriorates. An arterial blood gas is drawn. On room air at sea level, PaO2 is 68 mmHg and PaCO2 is 34 mmHg. Induced sputum samples reveal organisms on methenamine silver stain. What is the best treatment strategy for this patient?
A 26-year-old woman is brought to the emergency department after a suicide attempt. Her mother found her next to an empty bottle of acetaminophen in the bathroom. The patient reports that she ingested about twenty-five 500 mg pills. She took the pills 1 hour prior to arrival to the emergency department. She has a history of major depressive disorder. She does not smoke or use illicit drugs. Current medications include fluoxetine. She is oriented to person, place, and time. Vital signs are within normal limits. Physical examination shows no abnormalities. Laboratory studies show: Hemoglobin 12.5 g/dL Leukocyte count 8,000/mm3 Platelet count 150,000/mm3 Serum Prothrombin time 10.5 sec (INR=1.0) Na+ 141 mEq/L K+ 4.2 mEq/L Cl- 101 mEq/L HCO3- 25 mEq/L Urea nitrogen 10 g/dL Creatinine 0.5 g/dL Ca2+ 8.8 mg/dL Total bilirubin 0.4 mg/dL AST 22 U/L ALT 25 U/L Alkaline phosphatase 62 U/L Which of the following is the most appropriate next step in management?
A 45-year-old female who recently immigrated to the United States presents to the community health clinic for episodes of disrupted vision. She is concerned because she knows several people from her hometown who went blind after having these episodes. Over the past several months, she also has developed itchy bumps on her back and lower extremities. Physical exam reveals black hyperpigmented nodules with edema and palpable lymphadenopathy, but is otherwise unremarkable without any visible discharge from the eyes. Her physician explains her underlying disease was likely transmitted by black flies. Which of the following is the most appropriate pharmacotherapy for this patient?
A 10-year-old girl is brought to the physician because of itching of the vulva and anal region for the past 2 weeks. She has difficulty sleeping because of the itching. Physical examination shows excoriation marks around the vulva and perianal region. There is minor perianal erythema, but no edema or fissures. Microscopy of an adhesive tape applied to the perianal region shows multiple ova. Which of the following is the most appropriate treatment for this patient?
A 23-year-old woman visits her general practitioner with left ear pain and fever. She complains of multiple episodes of respiratory infection including bronchitis, laryngitis, and sinusitis. She was diagnosed with systemic lupus erythematosus with nephritis 8 months ago and was placed on oral prednisone. Currently, she takes prednisone daily. Her vital signs are as follows: blood pressure 130/85 mm Hg, heart rate 79/min, respiratory rate 16/min, and temperature 37.5°C (99.5°F). Her weight is 78 kg (172 lb) and height is 169 cm (5 ft 6 in). Physical examination reveals a swollen erythematous left eardrum, erythematous macular rash over sun-exposed skin, and slight calf edema. Inhibition of which of the following pathways causes diminished immune cell activation in this patient?
A 44-year-old woman is being treated by her oncologist for metastatic breast cancer. The patient had noticed severe weight loss and a fixed breast mass over the past 8 months but refused to see a physician until her husband brought her in. Surgery is scheduled, and the patient is given an initial dose of radiation therapy to destroy malignant cells. Which of the following therapies was administered to this patient?
An 84-year-old man comes to the emergency department because of lower back pain and lower extremity weakness for 3 weeks. Over the past week, he has also found it increasingly difficult to urinate. He has a history of prostate cancer, for which he underwent radical prostatectomy 8 years ago. His prostate-specific antigen (PSA) level was undetectable until a routine follow-up visit last year, when it began to increase from 0.8 ng/mL to its present value of 64.3 ng/mL (N < 4). An MRI of the spine shows infiltrative vertebral lesions with a collapse of the L5 vertebral body, resulting in cord compression at L4–L5. The patient receives one dose of intravenous dexamethasone and subsequently undergoes external beam radiation. Which of the following cellular changes is most likely to occur as a result of this treatment?
Practice by Chapter
Antiparasitic drugs (antiprotozoals)
Practice Questions
Antimalarial medications
Practice Questions
Anthelmintics
Practice Questions
Antiseptics and disinfectants
Practice Questions
Antimicrobial stewardship principles
Practice Questions
Empiric antimicrobial selection
Practice Questions
Antimicrobial dosing in special populations
Practice Questions
Antimicrobial pharmacokinetics/pharmacodynamics
Practice Questions
Antimicrobial toxicities
Practice Questions
Antimicrobial allergies and cross-reactivity
Practice Questions
Combination antimicrobial therapy
Practice Questions
Cost-effective antimicrobial strategies
Practice Questions
New antimicrobial development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app