
Antimicrobials — MCQs

On this page
A 2-year-old girl is rushed to the emergency department by her parents following ingestion of unknown pills from an unmarked bottle she found at the park. The parents are not sure how many pills she ingested but say the child has been short of breath since then. Her respiratory rate is 50/min and pulse is 150/min. Examination shows the girl to be quite restless and agitated. No other findings are elicited. Laboratory testing shows: Serum electrolytes Sodium 142 mEq/L Potassium 4.0 mEq/L Chloride 105 mEq/L Bicarbonate 14 mEq/L Serum pH 7.23 The girl most likely ingested which of the following drugs?
A 55-year-old woman with diabetes presents to the emergency department due to swelling of her left leg, fever, and chills for the past 2 days. The woman’s maximum recorded temperature at home was 38.3°C (101.0°F). Her left leg is red and swollen from her ankle to the calf, with an ill-defined edge. Her vital signs include: blood pressure 120/78 mm Hg, pulse rate 94/min, temperature 38.3°C (101.0°F), and respiratory rate 16/min. On physical examination, her left leg shows marked tenderness and warmth compared with her right leg. The left inguinal lymph node is enlarged to 3 x 3 cm. Which of the following chemical mediators is the most likely cause of the woman’s fever?
An American pediatrician travels to Bangladesh on a medical mission. While working in the local hospital's emergency room, she sees a 2-week-old boy who was brought in by his mother with muscle spasms and difficulty sucking. The mother gave birth at home at 38 weeks gestation and was attended to by her older sister who has no training in midwifery. The mother had no prenatal care. She has no past medical history and takes no medications. The family lives on a small fishing vessel on a major river, which also serves as their fresh water supply. The boy's temperature is 99°F (37.2°C), blood pressure is 100/60 mmHg, pulse is 130/min, and respirations are 22/min. On exam, the boy's arms are flexed at the elbow, his knees are extended, and his neck and spine are hyperextended. Tone is increased in the bilateral upper and lower extremities. He demonstrates sustained facial muscle spasms throughout the examination. The umbilical stump is foul-smelling. Cultures are taken, and the appropriate treatment is started. This patient's condition is most likely caused by a toxin with which of the following functions?
A 55-year-old male presents to his primary care physician for a normal check-up. He has a history of atrial fibrillation for which he takes metoprolol and warfarin. During his last check-up, his international normalized ratio (INR) was 2.5. He reports that he recently traveled to Mexico for a business trip where he developed a painful red rash on his leg. He was subsequently prescribed an unknown medication by a local physician. The rash resolved after a few days and he currently feels well. His temperature is 98.6°F (37°C), blood pressure is 130/80 mmHg, pulse is 95/min, and respirations are 18/min. Laboratory analysis reveals that his current INR is 4.5. Which of the following is the most likely medication this patient took while in Mexico?
A 17-year-old girl is brought to the emergency department 6 hours after she attempted suicide by consuming 16 tablets of acetaminophen (500 mg per tablet). At present, she does not have any complaints or symptoms. The patient is afebrile and vital signs are within normal limits. Physical examination is unremarkable. Laboratory findings show a serum acetaminophen level that is predictive of ‘probable hepatic toxicity’ on the Rumack-Matthew nomogram. Treatment is started with a drug, which is a precursor of glutathione and is a specific antidote for acetaminophen poisoning. Which of the following is an additional beneficial mechanism of action of this drug in this patient?
A 32-year-old woman is admitted to the hospital after undergoing an open cholecystectomy under general anesthesia. Preoperatively, the patient was administered a single dose of intravenous ceftriaxone. Now, the anesthetic effects have worn off, and her pain is well managed. The patient has a prior medical history of hypertension which has been well-controlled by captopril for 2 years. Her vitals currently show: blood pressure 134/82 mm Hg, heart rate 84/min, and respiratory rate 16/min. Postoperative laboratory findings are significant for the following: Serum glucose (random) 174 mg/dL Serum electrolytes Sodium 142 mEq/L Potassium 3.9 mEq/L Chloride 101 mEq/L Serum creatinine 0.9 mg/dL Blood urea nitrogen 10 mg/dL Alanine aminotransferase (ALT) 150 U/L Aspartate aminotransferase (AST) 172 U/L Serum bilirubin (total) 0.9 mg/dL Preoperative labs were all within normal limits. Which of the following drugs is most likely responsible for this patient’s abnormal laboratory findings?
A 13-year-old girl is brought to the physician because of an itchy rash on her knee and elbow creases. She has had this rash since early childhood. Physical examination of the affected skin shows crusty erythematous papules with skin thickening. She is prescribed topical pimecrolimus. The beneficial effect of this drug is best explained by inhibition of which of the following processes?
A 57-year-old man comes to the emergency department because of pain in the sides of his abdomen and blood-tinged urine since the previous night. Over the last 2 days, he has also had progressive malaise, myalgia, and a generalized itchy rash. He has a history of gastroesophageal reflux that did not respond to ranitidine but has improved since taking pantoprazole 2 months ago. He occasionally takes acetaminophen for back pain. His vital signs are within normal limits. Examination shows a generalized, diffuse maculopapular rash. The remainder of the examination shows no abnormalities. Laboratory studies show: Hemoglobin 13 g/dL Leukocyte count 7,800/mm3 Serum Na+ 140 mEq/L Cl- 105 mEq/L K+ 4.6 mEq/L HCO3- 25 mEq/L Glucose 102 mg/dL Creatinine 4.1 mg/dL Renal ultrasonography shows no abnormalities. Which of the following findings is most likely to be observed in this patient?
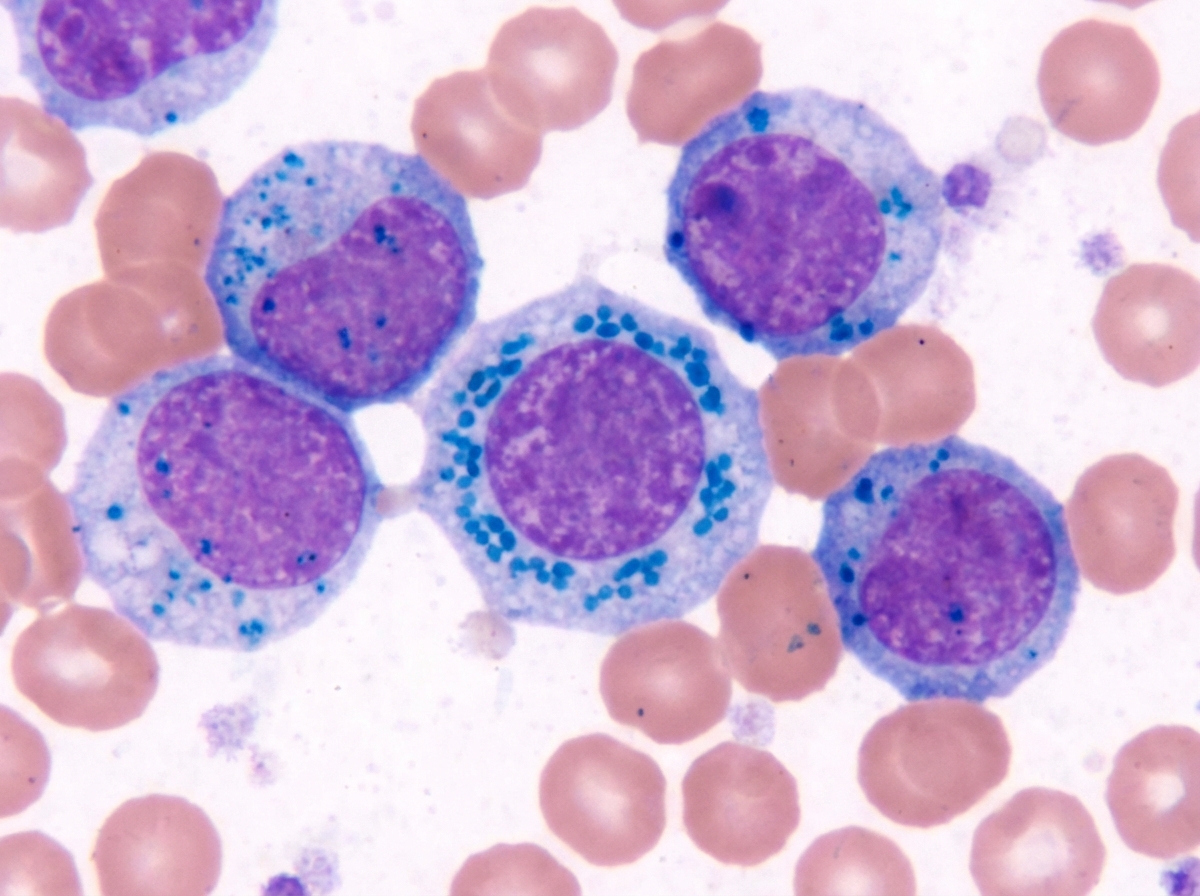
A 29-year-old Mediterranean man presents to the clinic for fatigue and lightheadedness for the past week. He reports an inability to exercise as his heart would beat extremely fast. He was recently diagnosed with active tuberculosis and started on treatment 2 weeks ago. He denies fever, weight loss, vision changes, chest pain, dyspnea, or bloody/dark stools. A physical examination is unremarkable. A Prussian blue-stained bone marrow aspirate is shown in figure A. What is the most likely explanation for this patient's symptoms?
A 57-year-old patient comes to the physician for a 2-month history of progressive dyspnea and cough productive of large amounts of yellow, blood-tinged sputum. He has a history of COPD and recurrent upper respiratory tract infections. Examination of the lung shows bilateral crackles and end-expiratory wheezing. An x-ray of the chest shows thin-walled cysts and tram-track opacities in both lungs. The physician prescribes nebulized N-acetylcysteine. Which of the following is the most likely effect of this drug?
Practice by Chapter
Antiparasitic drugs (antiprotozoals)
Practice Questions
Antimalarial medications
Practice Questions
Anthelmintics
Practice Questions
Antiseptics and disinfectants
Practice Questions
Antimicrobial stewardship principles
Practice Questions
Empiric antimicrobial selection
Practice Questions
Antimicrobial dosing in special populations
Practice Questions
Antimicrobial pharmacokinetics/pharmacodynamics
Practice Questions
Antimicrobial toxicities
Practice Questions
Antimicrobial allergies and cross-reactivity
Practice Questions
Combination antimicrobial therapy
Practice Questions
Cost-effective antimicrobial strategies
Practice Questions
New antimicrobial development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app