
Antimicrobials — MCQs

On this page
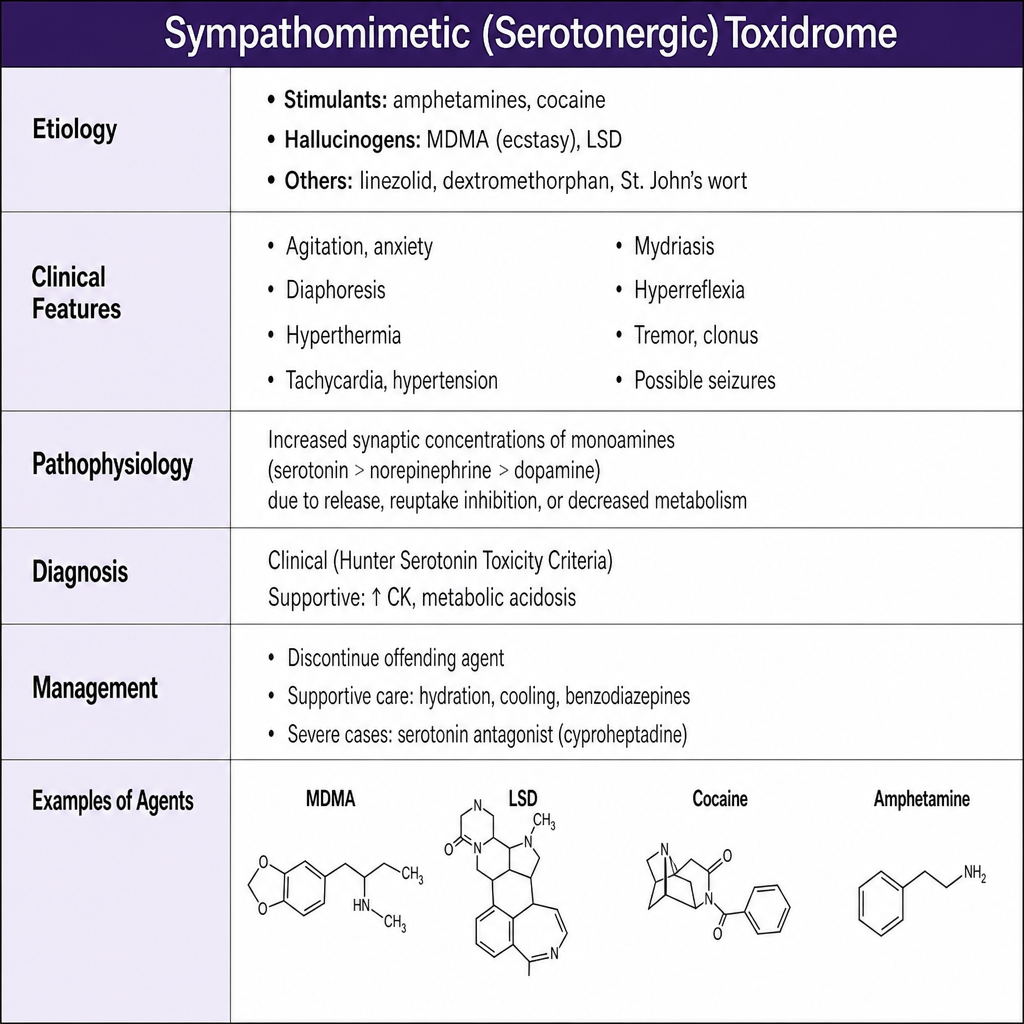
A 19-year-old woman is brought to the emergency department after ingesting an unknown substance at a party. On examination she is agitated, diaphoretic, and tachycardic (HR 138 bpm). Her pupils are 7 mm and reactive. Temperature is 39.8°C. She has hyperreflexia and bilateral ankle clonus. Which of the following agents is most likely responsible for this clinical picture?
A tourist with a travel history to India presents with complaints of abdominal pain and multiple episodes of watery diarrhea. He reports having food at a local restaurant the previous night. Which of the following antidiarrheal agents is used in this condition?
A patient from a North-Eastern state was diagnosed to have an infection with P. Falciparum malaria. What is the most appropriate treatment for this patient?
Which of the following chelating agents is indicated in iron overdose?
An 18-year-old boy from Rajasthan weighing 50 kg is diagnosed with mixed P . vivax and P . falciparum malaria. What is the appropriate treatment regimen on day 2?
In which phase of clinical trials is drug dosing typically determined?
Which of the following statements about Ciclesonide is incorrect?
Which of the following drugs, when given with erythromycin, can cause QT prolongation and Torsades de Pointes?
Which of the following is an inclusion criterion for the shorter bedaquiline regimen in the treatment of tuberculosis?
Aprepitant is a drug used in the treatment of some cases of chemotherapy-induced nausea and vomiting. What is the mechanism of action of this drug?
Practice by Chapter
Antiparasitic drugs (antiprotozoals)
Practice Questions
Antimalarial medications
Practice Questions
Anthelmintics
Practice Questions
Antiseptics and disinfectants
Practice Questions
Antimicrobial stewardship principles
Practice Questions
Empiric antimicrobial selection
Practice Questions
Antimicrobial dosing in special populations
Practice Questions
Antimicrobial pharmacokinetics/pharmacodynamics
Practice Questions
Antimicrobial toxicities
Practice Questions
Antimicrobial allergies and cross-reactivity
Practice Questions
Combination antimicrobial therapy
Practice Questions
Cost-effective antimicrobial strategies
Practice Questions
New antimicrobial development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app