
Antihypertensives — MCQs

On this page
An 81-year-old man with a history of congestive heart failure presents to his cardiologist because he has been feeling increasingly short of breath while lying down. Specifically, he says that he is now no longer able to sleep flat on the bed and instead has to be propped up on multiple pillows. In addition, he has been experiencing increased swelling in his legs. Finally, he reports that he has been experiencing muscle cramping and weakness. He reports that he has been taking a diuretic as prescribed and adhering to a low-salt diet. Physical exam reveals crackles on lung auscultation bilaterally and 2+ pitting edema in his legs bilaterally. Left ventricular ejection fraction (LVEF) is measured by echocardiogram and found to be 36%. This is decreased from his last measurement of 41%. He is put on a second diuretic that has an additional effect that corrects an electrolyte imbalance in this patient. Which of the following medications is consistent with this description?
A 67-year-old man with a history of diabetes mellitus type II and a previous myocardial infarction presents to your office for a routine examination. His blood pressure is found to be 180/100 mmHg. Which drug is the first-line choice of treatment for this patient's hypertension?
A 51-year-old woman comes to the physician because of a 6-month history of fatigue and increased thirst. She has no history of serious medical illness and takes no medications. She is 163 cm (5 ft 4 in) tall and weighs 72 kg (160 lb); BMI is 28 kg/m2. Her fasting serum glucose concentration is 249 mg/dL. Treatment with an oral hypoglycemic agent is begun. Which of the following best describes the mechanism of action of the drug that was most likely prescribed for this patient?
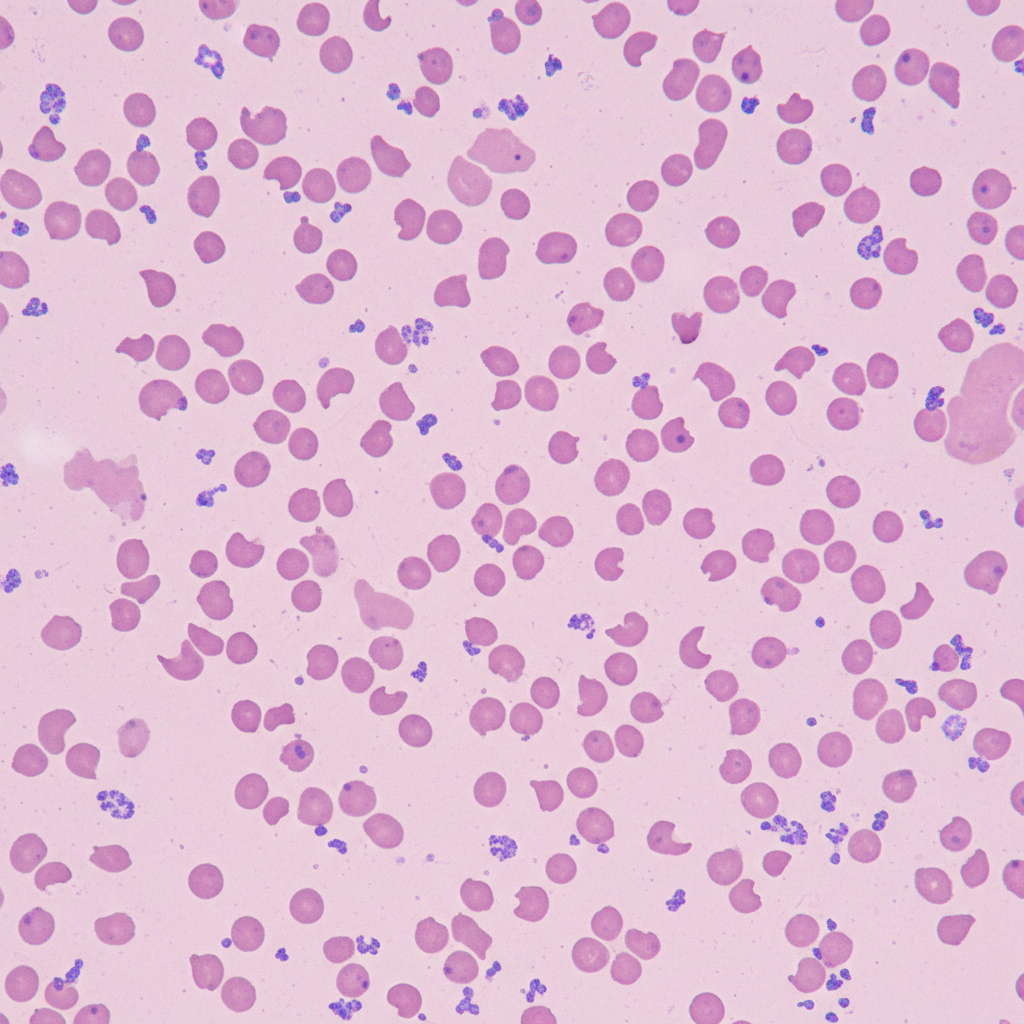
A 51-year-old woman is brought to the emergency department after not being able to urinate for the past 12 hours. She also complains of a headache that is sharp in nature, 9/10, without radiation, and associated with nausea and vomiting. She neither smokes cigarettes nor drinks alcohol. She complains that her fingers have become numb and very painful on exposure to cold weather during the last few months. She has also noticed her fingers change color from blue to pale to red on cold exposure. Her face looks shiny with thickened, wrinkle-free skin. She has had joint pain and stiffness for the last 20 years. She takes over-the-counter omeprazole for heartburn, which she says improves her symptoms. She has unintentionally lost 9 kg (20 lb) in the last 6 months. She has no previous history of diabetes, hypertension, chest pain, orthopnea, or paroxysmal nocturnal dyspnea. Her mother has rheumatoid arthritis for which she takes methotrexate, and her father takes medications for hypertension and hypercholesterolemia. Her temperature is 37°C (98.6°F), blood pressure is 210/120 mm Hg, pulse is 102/min, respiratory rate is 18/min, and BMI is 22 kg/m2. Laboratory test Complete blood count: Hemoglobin 9.5 g/dL Leukocytes 15,500/mm3 Platelets 90,000/mm3 Serum haptoglobin 20 mg/dL (30–200 mg/dL) Serum creatinine 2.3 mg/dL Blood urea nitrogen 83.5 mg/dL The peripheral blood film of the patient shows the following. Which of the following would be the most appropriate treatment for this patient?
A 45-year-old diabetic man presents to your office for routine follow-up. One year ago, the patient’s hemoglobin A1C was 7.2% and the patient was encouraged to modify his diet and increase exercise. Six months ago, the patient’s HA1C was 7.3%, and you initiated metformin. Today, the patient has no complaints. For which of the following co-morbidities would it be acceptable to continue metformin?
A 45-year-old woman presents to your office with a serum glucose of 250 mg/dL and you diagnose diabetes mellitus type II. You intend to prescribe the patient metformin, but you decide to order laboratory tests before proceeding. Which of the following basic metabolic panel values would serve as a contraindication to the use of metformin?
A 57-year-old woman comes to the physician because of a 2-week history of swelling of both her feet. It improves a little bit with elevation but is still bothersome to her because her shoes no longer fit. She has type 2 diabetes mellitus treated with metformin and linagliptin. She was diagnosed with hypertension 6 months ago and started treatment with amlodipine. Subsequent blood pressure measurements on separate occasions have been around 130/90 mm Hg. She otherwise feels well. Today, her pulse is 80/min, respirations are 12/min, and blood pressure is 132/88 mm Hg. Cardiovascular examination shows no abnormalities. There is pitting edema of both ankles. Which of the following would have been most likely to reduce the risk of edema in this patient?
A 58-year-old male presents to the clinic for a follow-up visit. He takes metformin every day and says that he is compliant with his medication but can not control his diet. Three months prior, his HbA1c was 8.2% when he was started on metformin. He does not have any complaints on this visit. His temperature is 37°C (98.6°F), respirations are 15/min, pulse is 67/min and blood pressure is 122/88 mm Hg. His BMI is 33. Physical examination is within normal limits. Blood is drawn for laboratory tests and the results are given below: Fasting blood glucose 150 mg/dL Glycated hemoglobin (HbA1c) 7.2 % Serum Creatinine 1.1 mg/dL BUN 12 mg/dL The physician wants to initiate another medication for his blood glucose control, specifically one that does not carry a risk of weight gain. Addition of which of the following drugs would be most suitable for this patient?
A 54-year-old African American male presents to the emergency department with 1 day history of severe headaches. He has a history of poorly controlled hypertension and notes he hasn't been taking his antihypertensive medications. His temperature is 100.1 deg F (37.8 deg C), blood pressure is 190/90 mmHg, pulse is 60/min, and respirations are 15/min. He is started on a high concentration sodium nitroprusside infusion and transferred to the intensive care unit. His blood pressure eventually improves over the next two days and his headache resolves, but he becomes confused and tachycardic. Labs reveal a metabolic acidosis. Which of the following is the best treatment?
A 58-year-old woman presents to her physician complaining of a headache in the occipital region for 1 week. Past medical history is significant for essential hypertension, managed with lifestyle modifications and 2 antihypertensives for the previous 6 months. Her blood pressure is 150/90 mm Hg. Neurological examination is normal. A third antihypertensive drug is added that acts as a selective α2 adrenergic receptor agonist. On follow-up, she reports that she does not have any symptoms and her blood pressure is 124/82 mm Hg. Which of the following mechanisms best explains the therapeutic effect of this new drug in this patient?
Practice by Chapter
Diuretic classes and mechanisms
Practice Questions
ACE inhibitors
Practice Questions
Angiotensin II receptor blockers
Practice Questions
Calcium channel blockers (dihydropyridine/non-dihydropyridine)
Practice Questions
Beta-blockers (cardioselective/non-selective)
Practice Questions
Alpha-blockers
Practice Questions
Alpha-2 agonists
Practice Questions
Direct vasodilators
Practice Questions
Direct renin inhibitors
Practice Questions
SGLT2 inhibitors in hypertension
Practice Questions
Mineralocorticoid receptor antagonists
Practice Questions
Combination antihypertensive therapy
Practice Questions
Resistant hypertension management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app