
Antihypertensives — MCQs

On this page
A 45-year-old woman presents to a physician with repeated episodes of vertigo for the last 6 months. The episodes usually last for 20–30 minutes, but 2 episodes persisted for more than an hour. The episodes are often associated with severe nausea and vomiting. She has experienced falls after losing her balance during these episodes on 3 occasions, but she has never lost consciousness. However, she reports that after an acute episode is over, she feels unsteady, tired, and nauseated for several hours. For the previous month, she has noted that the acute attacks of vertigo are preceded by a sense of fullness in the ear, hearing an ocean-like roaring sound, and hearing loss on the left side. In between episodes, she is completely normal. There is no history of a known medical disorder, substance use or regular use of medications. The vital signs are within normal limits. The neurologic examination shows normal tone and power in all muscle groups, normal deep tendon reflexes, absence of signs of cerebellar dysfunction, and normal gait. The Dix-Hallpike positional test is negative. The otoscopic exam of both ears does not reveal any significant abnormality. The physician orders an audiogram, which suggests mild low-frequency sensorineural hearing loss on the left side. In addition to lifestyle changes and symptomatic treatment of acute episodes, which of the following is the most appropriate initial treatment to prevent recurrent episodes?
A 38-year-old man is brought to the emergency department 35 minutes after an episode of loss of consciousness. He was having dinner with a client when his left arm suddenly became weak and numb. A few minutes later he became tense and his arms and legs began jerking violently, following which he lost consciousness. He has no recollection of this event. He works as a business consultant. He has a history of asthma and major depressive disorder. Current medication include an albuterol inhaler and doxepin. He increased the dose of doxepin one week ago because he felt the medication was not helping. He drinks two to three beers on the weekend. He admits to using cocaine 4–5 times per week. On arrival, he is alert and oriented to person, place, and time. His speech is slurred. His temperature is 37°C (98.6F), pulse is 96/min, and blood pressure is 155/90 mm Hg. The pupils are equal and reactive to light. Neurologic exam shows left facial droop. There is 3/5 strength in the left arm. Which of the following is the most likely underlying mechanism of this patient's symptoms?
A 53-year-old woman presents to a physician for a regular check-up. She has no complaints, but notes that she has been anxious and easily irritable for no particular reason over the past year. Six months ago, she was diagnosed with grade I arterial hypertension and prescribed lifestyle modification and weight loss to control her blood pressure. She currently takes aspirin (81 mg) and rosuvastatin (10 mg) daily. The vital signs are as follows: blood pressure 145/80 mm Hg, heart rate 81/min, respiratory rate 14/min, and temperature 36.6℃ (97.9℉). She weighs 91 kg (213.8 lb), the height is 167 cm (5.5 ft), and the BMI is 32.6 kg/m2. The physical examination is unremarkable. Blood testing was performed, and the results are shown below. Plasma glucose 109.9 mg/dL (6.1 mmol/L) Plasma triglycerides 185.8 mg/dL (2.1 mmol/L) Na+ 141 mEq/L K+ 4.2 mEq/L The patient was prescribed atenolol. If the medication alone affects the patient’s measurements, which laboratory finding would you expect to note several weeks after the treatment is initiated?
A 58-year-old male with a history of congestive heart failure and hypertension comes to you with the chief complaint of new-onset cough as well as increased serum potassium in the setting of a new medication. Which of the following medications is most likely responsible for these findings?
A new drug has been shown to block epithelial sodium channels in the cortical collecting duct. Which of the following is most likely to be decreased upon drug administration?
A 1-week-old male newborn is brought to the physician for the evaluation of persistent irritability and crying. He was born at 36 weeks' gestation. Pregnancy was complicated by polyhydramnios. His mother reports that she nurses him frequently and changes his diapers 18–20 times per day. He is at the 5th percentile for length and 10th percentile for weight. Physical examination shows a triangular face with a prominent forehead and large, protruding ears. Serum studies show: Na+ 129 mEq/L K+ 2.8 mEq/L Cl- 90 mEq/L Ca2+ 8.0 mg/dL HCO3- 32 mEq/L Arterial blood gas analysis shows a pH of 7.51. The effects of this patient's condition are most similar to the long-term administration of which of the following drugs?
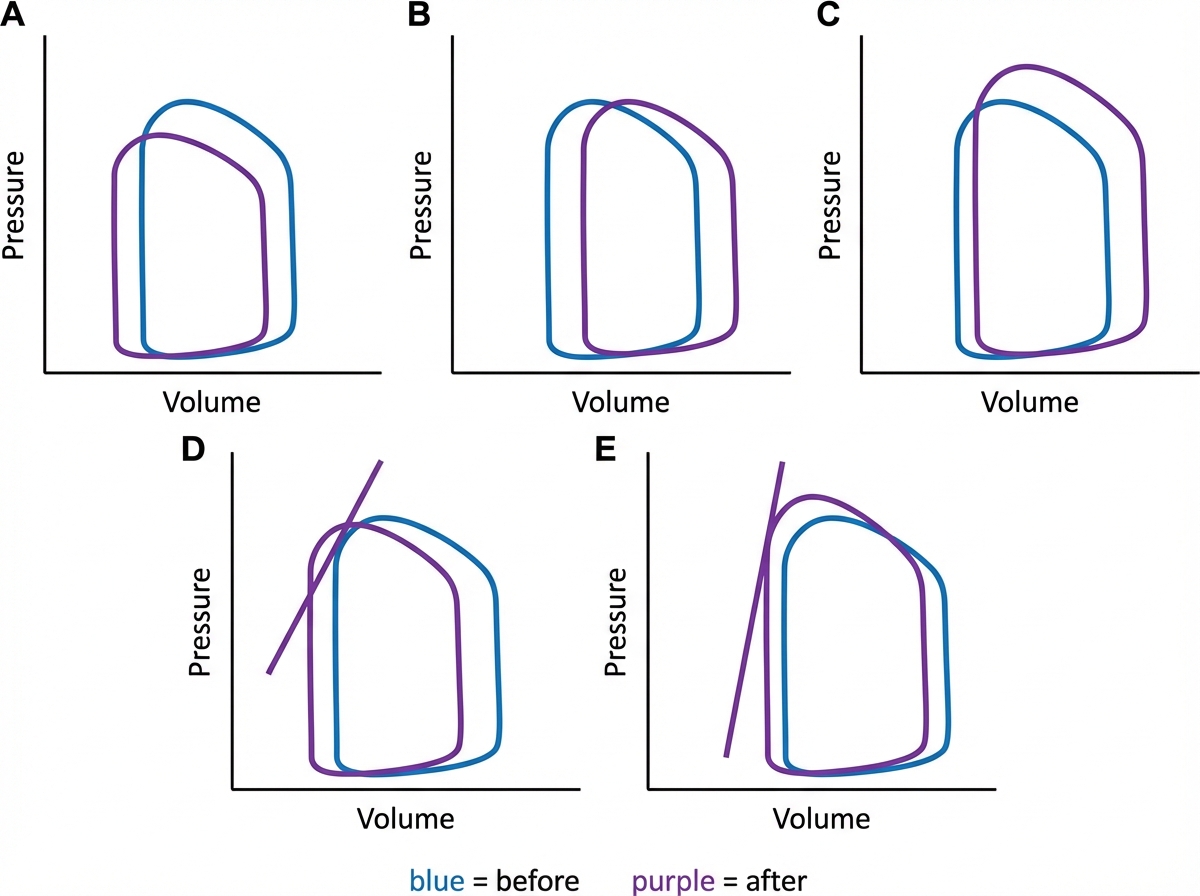
A 55-year-old man presents to the emergency department complaining of mild vision changes, dizziness, and severe pain in the chest for the past hour. He has also been experiencing nausea since this morning and has already vomited twice. Past medical history includes poorly controlled type 2 diabetes and end-stage renal disease requiring dialysis. His blood pressure is 210/100 mm Hg, pulse is 110/min, and respirations are 18/min. Ophthalmic examination of his eyes show papilledema and flame-shaped hemorrhages and he is diagnosed with hypertensive emergency. Treatment involves rapidly lowering his blood pressure, and he is started on intravenous sodium nitroprusside while emergent dialysis is arranged. Which of the following cardiac pressure-volume loops closely represents the action of the drug he has been administered, where blue represents before administration and purple represent after administration?
A 54-year-old woman comes to the physician for a follow-up examination after presenting with elevated blood pressure readings during her last two visits. After her last visit 2 months ago, she tried controlling her hypertension with weight loss before starting medical therapy, but she has since been unable to lose any weight. Her pulse is 76/min, and blood pressure is 154/90 mm Hg on the right arm and 155/93 mm Hg on the left arm. She agrees to start treatment with a thiazide diuretic. In response to this treatment, which of the following is most likely to decrease?
A 21-year-old male presents to the emergency department with generalized weakness and fatigue. His past medical history is significant for hypertension refractory to several medications but is otherwise unremarkable. He is afebrile, his pulse is 82/min, respirations are 18/min, and blood pressure is 153/94 mmHg. Labs are as follows: Sodium: 142 mEq/L Potassium: 2.7 mEq/L Bicarbonate: 36 mEq/L Serum pH: 7.5 pCO2: 50 mmHg Aldosterone: Decreased Based on clinical suspicion, a genetic screen is performed, confirming an underlying syndrome due to an autosomal dominant gain of function mutation. Which of the following medications can be given to treat the most likely cause of this patient's symptoms?
A 67-year-old gentleman with a history of poorly controlled diabetes presents to his primary care physician for a routine examination. He is found to be hypertensive on physical exam and is started on a medication that is considered first-line therapy for his condition. What should the physician warn the patient about before the patient takes his first dose of the medication?
Practice by Chapter
Diuretic classes and mechanisms
Practice Questions
ACE inhibitors
Practice Questions
Angiotensin II receptor blockers
Practice Questions
Calcium channel blockers (dihydropyridine/non-dihydropyridine)
Practice Questions
Beta-blockers (cardioselective/non-selective)
Practice Questions
Alpha-blockers
Practice Questions
Alpha-2 agonists
Practice Questions
Direct vasodilators
Practice Questions
Direct renin inhibitors
Practice Questions
SGLT2 inhibitors in hypertension
Practice Questions
Mineralocorticoid receptor antagonists
Practice Questions
Combination antihypertensive therapy
Practice Questions
Resistant hypertension management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app