
Calcium channel blockers (dihydropyridine/non-dihydropyridine) — MCQs

A molecular biologist is studying the roles of different types of ion channels regulating cardiac excitation. He identifies a voltage-gated calcium channel in the sinoatrial node, which is also present throughout the myocardium. The channel is activated at ~ -40 mV of membrane potential, undergoes voltage-dependent inactivation, and is highly sensitive to nifedipine. Which of the following phases of the action potential in the sinoatrial node is primarily mediated by ion currents through the channel that the molecular biologist is studying?
A 72-year-old man comes to the emergency department because of blurry vision for the past 3 days. He has also had 4 episodes of right-sided headaches over the past month. He has no significant past medical history. His father died of coronary artery disease at the age of 62 years. His temperature is 37.2°C (99°F), pulse is 94/min, and blood pressure is 232/128 mm Hg. Fundoscopy shows right-sided optic disc blurring and retinal hemorrhages. A medication is given immediately. Five minutes later, his pulse is 75/min and blood pressure is 190/105 mm Hg. Which of the following drugs was most likely administered?
A previously healthy 52-year-old woman comes to the physician because of a 3-month history of chest pain on exertion. She takes no medications. Cardiopulmonary examination shows no abnormalities. Cardiac stress ECG shows inducible ST-segment depressions in the precordial leads that coincide with the patient's report of chest pain and resolve upon cessation of exercise. Pharmacotherapy with verapamil is initiated. This drug is most likely to have which of the following sets of effects? $$$ End-diastolic volume (EDV) %%% Blood pressure (BP) %%% Contractility %%% Heart rate (HR) $$$
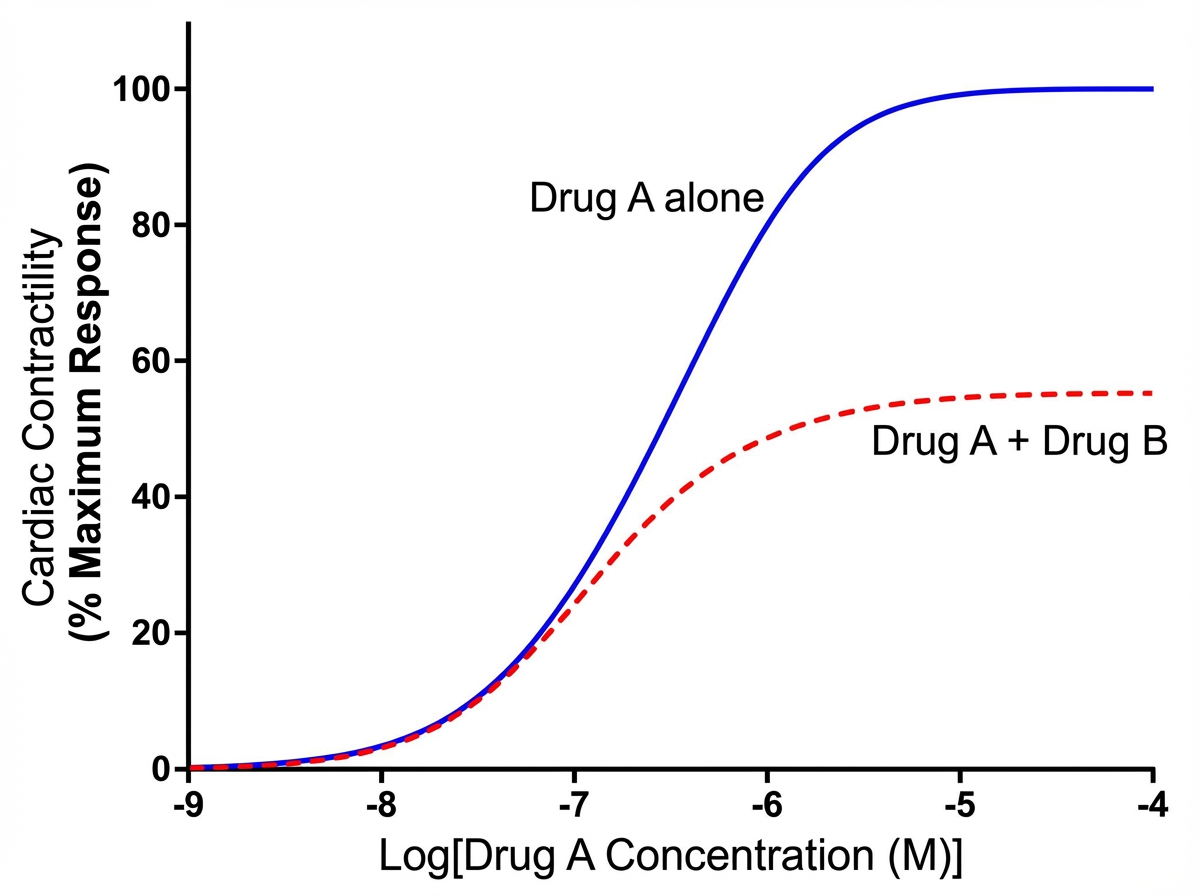
An investigator is studying the effects of different drugs on the contraction of cardiomyocytes. The myocytes are able to achieve maximal contractility with the administration of drug A. The subsequent administration of drug B produces the response depicted in the graph shown. Which of the following drugs is most likely to produce a response similar to that of drug B?
A previously healthy 45-year-old man comes to the physician for a routine health maintenance examination. He has been having recurrent headaches, especially early in the morning, and sometimes feels dizzy. There is no family history of serious illness. The patient runs 5 miles 3 days a week. He does not smoke or drink alcohol. He is 177 cm (5 ft 10 in) tall and weighs 72 kg (159 lb); BMI is 23 kg/m2. His temperature is 37°C (98.6°F), pulse is 70/min, and blood pressure is 152/90 mm Hg. Physical examination shows no abnormalities. Laboratory studies are within normal limits. Two weeks later, the patient's blood pressure is 150/90 mm Hg in both arms. He is started on an antihypertensive medication. One month later, physical examination shows 2+ pretibial edema bilaterally. This patient was most likely treated with which of the following medications?
A 44-year-old man comes to the emergency department because of a severe headache and blurry vision for the past 3 hours. He has hypertension treated with hydrochlorothiazide. He has missed taking his medication for the past week as he was traveling. He is only oriented to time and person. His temperature is 37.1°C (98.8°F), pulse is 92/min and regular, and blood pressure is 245/115 mm Hg. Cardiopulmonary examination shows no abnormalities. Fundoscopy shows bilateral retinal hemorrhages and exudates. Neurologic examination shows no focal findings. A complete blood count and serum concentrations of electrolytes, glucose, and creatinine are within the reference range. A CT scan of the brain shows no abnormalities. Which of the following is the most appropriate pharmacotherapy?
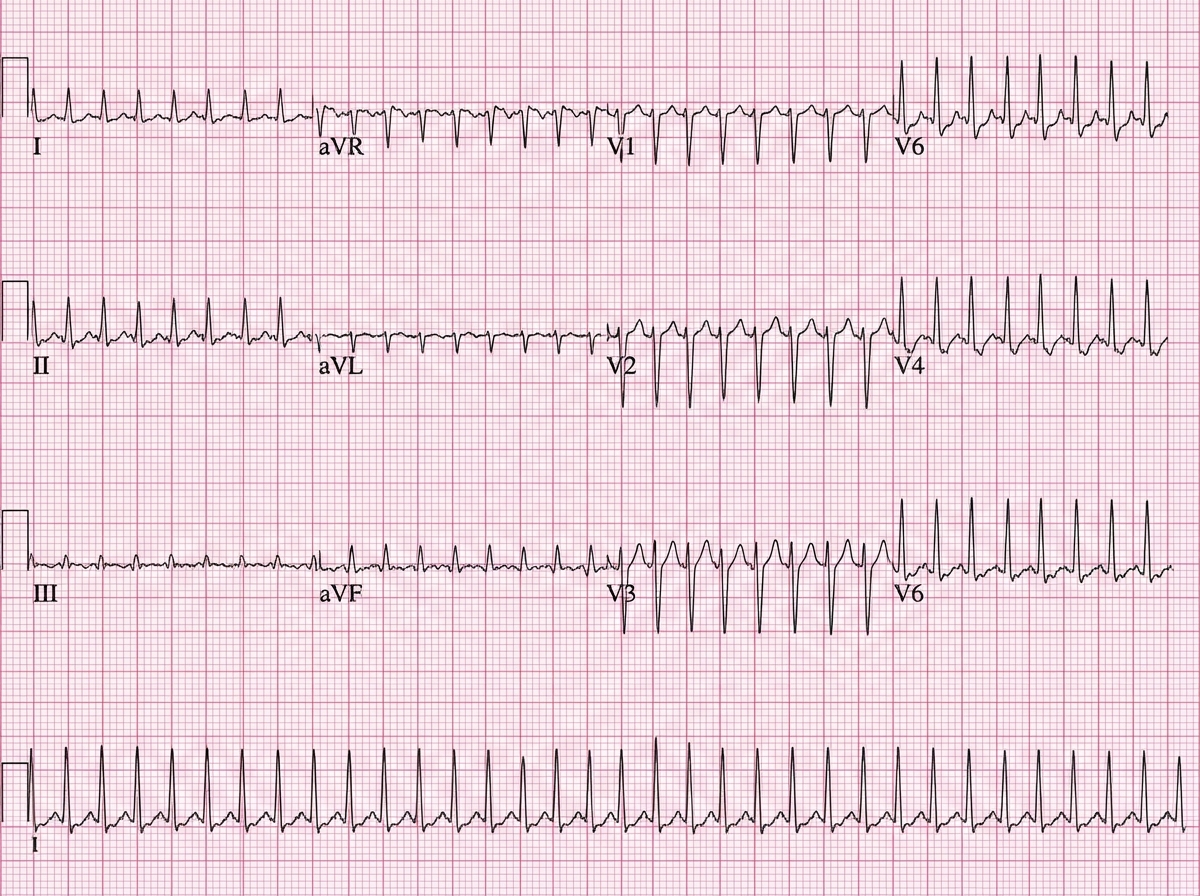
A 52-year-old man presents to the emergency department (ED) complaining of palpitations and lightheadedness for the last 30 minutes. He denies feeling pain or discomfort in his chest and is not short of breath. He does not have any known medical problems and does not take any medications regularly. He drinks 4–6 caffeinated drinks a day. The temperature is 36.8°C (98.2°F), the pulse rate is 150/min and slightly irregular, the blood pressure is 144/84 mm Hg, and the respiratory rate is 16/min. A focused examination of the cardiovascular and respiratory systems is unremarkable. An electrocardiogram is performed in the ED and the results are shown in the accompanying image. The ED physician prescribes a calcium channel blocking agent for his condition. Which of the following statements best describes the choice of verapamil over nifedipine in the treatment of this patient?
An 18-year-old boy is brought to the emergency department by his parents because he suddenly collapsed while playing football. His parents mention that he had complained of dizziness while playing before, but never fainted in the middle of a game. On physical examination, the blood pressure is 130/90 mm Hg, the respirations are 15/min, and the pulse is 110/min. The chest is clear, but a systolic ejection murmur is present. The remainder of the examination revealed no significant findings. An electrocardiogram is ordered, along with an echocardiogram. He is diagnosed with hypertrophic cardiomyopathy and the physician lists all the precautions he must follow. Which of the following drugs will be on the list of contraindicated substances?
A 27-year-old woman with no past medical history presents to her primary care provider because she has begun to experience color changes in her fingers on both hands in cold temperatures. She reports having had this problem for a few years, but with the weather getting colder this winter she has grown more concerned. She says that when exposed to cold her fingers turn white, blue, and eventually red. When the problem subsides she experiences pain in the affected fingers. She says that wearing gloves helps somewhat, but she continues to experience the problem. Inspection of the digits is negative for ulcerations. Which of the following is the next best step in treatment?
A 65-year-old male with a history of hypertension presents to his primary care physician complaining of multiple episodes of chest pain, palpitations, and syncope. Episodes have occurred twice daily for the last week, and he is asymptomatic between episodes. Electrocardiogram reveals a narrow-complex supraventricular tachycardia. He is treated with diltiazem. In addition to its effects on cardiac myocytes, on which of the following channels and tissues would diltiazem also block depolarization?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app