
Beta-blockers (cardioselective/non-selective) — MCQs

A 34-year-old female presents to the emergency room with headache and palpitations. She is sweating profusely and appears tremulous on exam. Vital signs are as follows: HR 120, BP 190/110, RR 18, O2 99% on room air, and Temp 37C. Urinary metanephrines and catechols are positive. Which of the following medical regimens is contraindicated as a first-line therapy in this patient?
A 55-year-old woman comes to the physician because of involuntary hand movements that improve with alcohol consumption. Physical examination shows bilateral hand tremors that worsen when the patient is asked to extend her arms out in front of her. The physician prescribes a medication that is associated with an increased risk of bronchospasms. This drug has which of the following immediate effects on the cardiovascular system? Stroke volume | Heart rate | Peripheral vascular resistance
A 55-year-old man comes to the physician because of episodic retrosternal chest pain and shortness of breath for the past 6 months. His symptoms occur when he takes long walks or climbs stairs but resolve promptly with rest. He has a history of chronic obstructive pulmonary disease, for which he takes ipratropium bromide. His pulse is 81/min and blood pressure is 153/82 mm Hg. Physical examination shows mild expiratory wheezing over both lungs. Additional treatment with a beta blocker is considered. Which of the following agents should be avoided in this patient?
A 65-year-old male with a history of CHF presents to the emergency room with shortness of breath, lower leg edema, and fatigue. He is diagnosed with acute decompensated congestive heart failure, was admitted to the CCU, and treated with a medication that targets beta-1 adrenergic receptors preferentially over beta-2 adrenergic receptors. The prescribing physician explained that this medication would only be used temporarily as its efficacy decreases within 2-3 days due to receptor downregulation. Which of the following was prescribed?
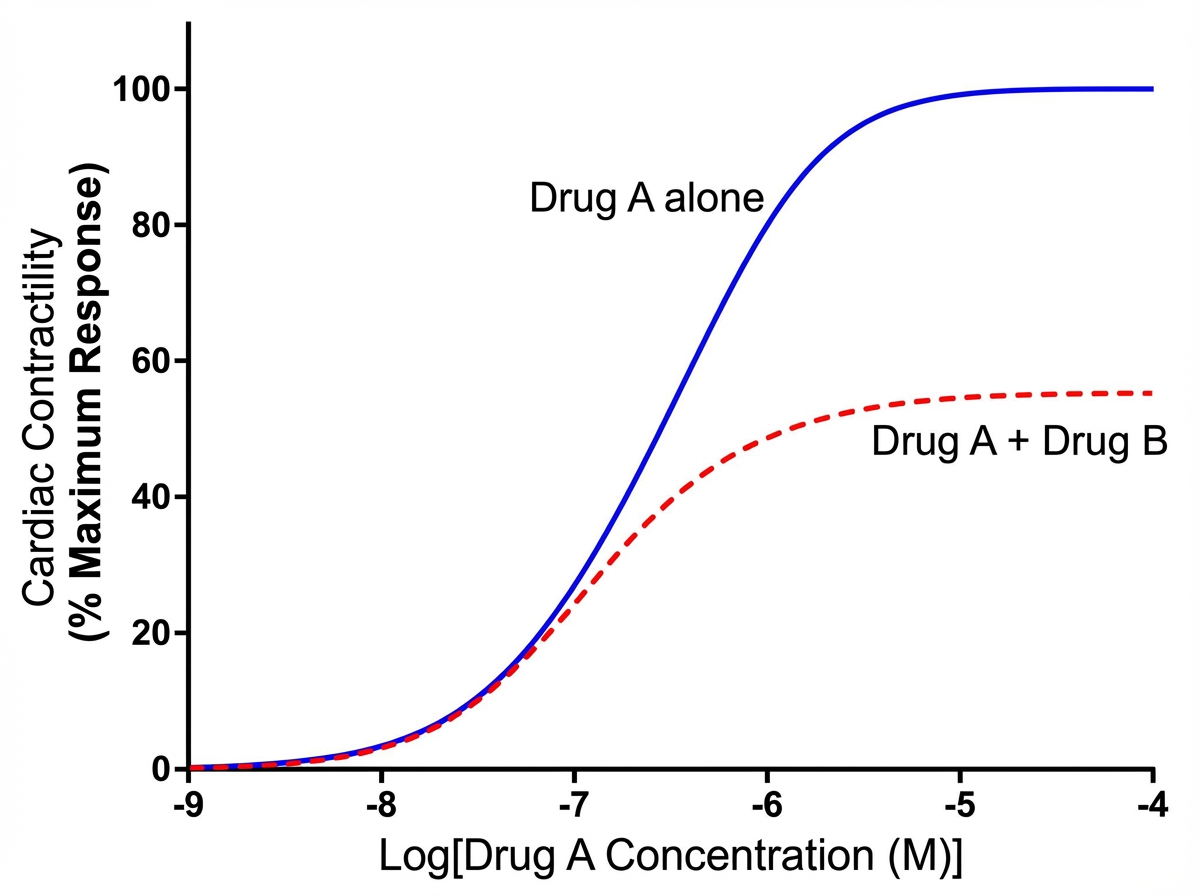
An investigator is studying the effects of different drugs on the contraction of cardiomyocytes. The myocytes are able to achieve maximal contractility with the administration of drug A. The subsequent administration of drug B produces the response depicted in the graph shown. Which of the following drugs is most likely to produce a response similar to that of drug B?
A 61-year-old man with longstanding diabetes and coronary artery disease presents to the ER with chest pain and dyspnea. The echocardiogram reveals moderate-to-severe mitral regurgitation and an ejection fraction of 27%. A chest X-ray shows bibasilar infiltrates. A new drug is added to his medication regimen, and the physician mentions urinary frequency, increased breast tissue development, and erectile dysfunction as possible side effects. What is the mechanism of action of this drug?
A 48-year-old man presents to the emergency department with complaints of substernal chest pain for the past 1 hour. The pain is crushing in nature and radiates to his neck and left arm. He rates the pain as 7/10. He gives a history of similar episodes in the past that resolved with rest. He is a non-smoker and drinks alcohol occasionally. On physical examination, the temperature is 37.0°C (98.6°F), the pulse rate is 130/min and irregular, the blood pressure is 148/92 mm Hg, and the respiratory rate is 18/min. The physician immediately orders an electrocardiogram, the findings of which are consistent with an acute Q-wave myocardial infarction (MI). After appropriate emergency management, he is admitted to the medical floor. He develops atrial fibrillation on the second day of admission. He is given a β-adrenergic blocking agent for the arrhythmia. On discharge, he is advised to continue the medication for at least 2 years. Which of the following β-adrenergic blocking agents was most likely prescribed to this patient?
A 63-year-old woman presents with dyspnea on exertion. She reports that she used to work in her garden without any symptoms, but recently she started to note dyspnea and fatigue after working for 20–30 minutes. She has type 2 diabetes mellitus diagnosed 2 years ago but she does not take any medications preferring natural remedies. She also has arterial hypertension and takes torsemide 20 mg daily. The weight is 88 kg and the height is 164 cm. The vital signs include: blood pressure is 140/85 mm Hg, heart rate is 90/min, respiratory rate is 14/min, and the temperature is 36.6℃ (97.9℉). Physical examination is remarkable for increased adiposity, pitting pedal edema, and present S3. Echocardiography shows a left ventricular ejection fraction of 51%. The combination of which of the following medications would be a proper addition to the patient’s therapy?
A 23-year-old active college student has a sudden loss of consciousness 40 minutes after he was playing basketball with his team. Cardiopulmonary resuscitation is administered by bystanders. On arrival of emergency medical professionals, he regains his consciousness. He has no past medical history. He does not smoke or drink alcohol. His family history is positive for a cousin who died suddenly in his youth. On physical examination, a systolic ejection murmur is audible on the left lower sternal border. ECG shows left ventricular hypertrophy and echocardiography shows asymmetric septal hypertrophy. Which of the following decreases the pressure gradient between the aorta and the left ventricle in this patient?
A 72-year-old man presents to the outpatient clinic today. He has New York Heart Association class III heart failure. His current medications include captopril 20 mg, furosemide 40 mg, potassium chloride 10 mg twice daily, rosuvastatin 20 mg, and aspirin 81 mg. He reports that he generally feels well and has not had any recent worsening of his symptoms. His blood pressure is 132/85 mm Hg and heart rate is 84/min. Physical examination is unremarkable except for trace pitting edema of the bilateral lower extremities. What other medication should be added to his heart failure regimen?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app