
Antihypertensives — MCQs

On this page
A 25 -year-old male presented to the emergency department with head trauma due to a road traffic accident. In the hospital, the patient developed seizures, and an emergency CT scan revealed widespread cerebral edema. Which of the following is the diuretic of choice for cerebral edema in this patient?
A person was taking an antihypertensive drug and continued taking it despite developing constipation, dry mouth, and dizziness. He was taking it regularly but forgot to take it during a trip abroad and has now developed a hypertensive emergency. Which antihypertensive was he likely taking?
A patient presents with hypertension and has a history of renal stones, along with several episodes of renal colic. Which diuretic is the most appropriate to use?
Which of the following cardioselective betablockers has been shown to decrease mortality in patients with congestive heart failure?
A hypertensive patient wants to conceive. Which of the following medications needs to be stopped before pregnancy?
A patient with hypertension, peripheral edema, and chronic kidney disease (CKD) presents for management. Which of the following medications would be the best choice?
A 38-year-old male presents to his primary care doctor with 8 months of uncontrollable anxiety. He states that he experiences overwhelming anxiety and worry in performing just ordinary tasks of daily living. He is started on venlafaxine for treatment of generalized anxiety disorder. Which of the following is a potential side effect of this medication?
A 61-year-old woman presents to her primary care provider with complaints of fatigue, weight gain of 5.5 kg (12.1 lb) and intermittent nausea over the past 4 months. She denies any changes to her diet. She has had type 2 diabetes mellitus for the past 27 years complicated by diabetic neuropathy. Vital signs include: temperature 37.0°C (98.6°F), blood pressure 167/98 mm Hg and pulse 80/min. Physical examination reveals bilateral pitting lower-extremity edema. Fundoscopic examination reveals bilateral micro-aneurysms and cotton wool patches. Her serum creatinine is 2.6 mg/dL. Which of the following is the best initial therapy for this patient?
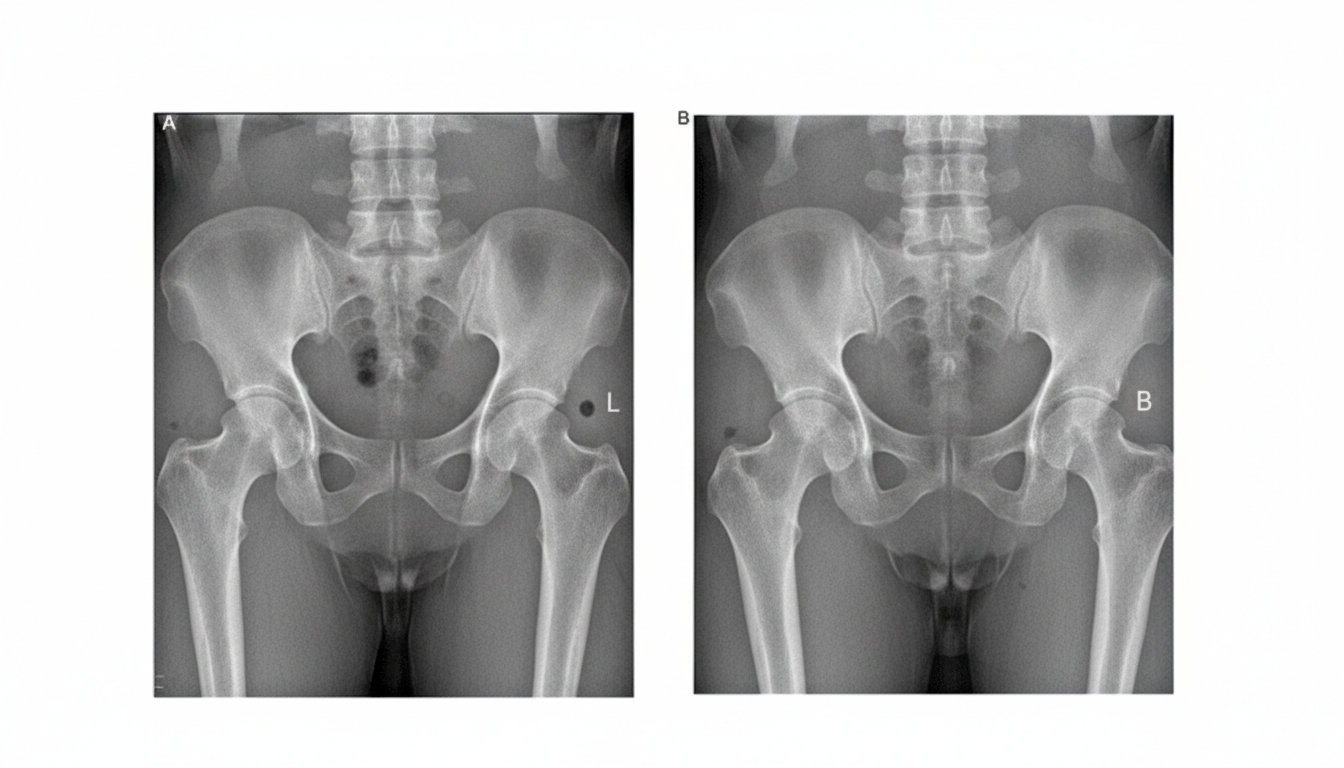
A 63-year-old woman presents to her physician with hip pain. She has had pain in both hips for almost 5 years, and it has progressed over time. She notes that it gets worse as the day goes on, making it difficult for her to walk her small dog in the evening. She has a little morning stiffness which subsides quickly after she starts to walk. In the last week, her pain became worse. The past medical history includes hypertension, hyperlipidemia, and mild hypothyroidism. She takes captopril, atorvastatin, and levothyroxine. She has also been taking acetaminophen almost every day with a dose increase up to 4,000 mg, but there is no significant decrease in pain. Both of her parents died in their 80's. The blood pressure is 135/85 mm Hg, heart rate is 74/min, respiratory rate is 12/min, and the temperature is 37.0°C (98.6°F). The BMI is 35 kg/m2. On physical examination, the leg strength is normal bilaterally. The neurological exam of both upper and lower extremities is normal. Her gait is difficult to assess due to pain. A radiograph of her left hip joint is shown in the image below. Which of the following is the most appropriate treatment for the patient’s condition?
A 56-year-old woman presents to the physician for a routine health maintenance examination. She has no history of a serious illness and takes no medications. She exercises every day and follows a healthy diet. She does not smoke and consumes alcohol moderately. There is no family history of chronic disease. Her blood pressure is 145/92 mm Hg, which is confirmed on a repeat measurement. Her BMI is 23 kg/m2. The physical examination shows no abnormal findings. The laboratory test results show: Serum Total cholesterol 193 mg/dL Low-density lipoprotein (LDL-C) 124 mg/dL High-density lipoprotein (HDL-C) 40 mg/dL Triglycerides 148 mg/dL Her 10-year risk of CVD is 3.6%. Antihypertensive medication is initiated for her elevated blood pressure. Which of the following is the most appropriate additional pharmacotherapy at this time?
Practice by Chapter
Diuretic classes and mechanisms
Practice Questions
ACE inhibitors
Practice Questions
Angiotensin II receptor blockers
Practice Questions
Calcium channel blockers (dihydropyridine/non-dihydropyridine)
Practice Questions
Beta-blockers (cardioselective/non-selective)
Practice Questions
Alpha-blockers
Practice Questions
Alpha-2 agonists
Practice Questions
Direct vasodilators
Practice Questions
Direct renin inhibitors
Practice Questions
SGLT2 inhibitors in hypertension
Practice Questions
Mineralocorticoid receptor antagonists
Practice Questions
Combination antihypertensive therapy
Practice Questions
Resistant hypertension management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app