
Vaccines — MCQs

On this page
A 4-month-old boy is brought to the physician by his parents for a well-child examination. He has cystic fibrosis diagnosed by newborn screening. His parents report frequent feedings and large-volume and greasy stools. His 4-year-old brother has autism. Current medications include bronchodilators, pancreatic enzyme supplements, and fat-soluble vitamins. He is at the 18th percentile for height and 15th percentile for weight. Scattered wheezes are heard throughout both lung fields. Examination shows a distended and tympanic abdomen with no tenderness or guarding. Which of the following is a contraindication for administering one or more routine vaccinations?
A 12-month-old girl is brought to her pediatrician for a checkup and vaccines. The patient’s mother wants to send her to daycare but is worried about exposure to unvaccinated children and other potential sources of infection. The toddler was born at 39 weeks gestation via spontaneous vaginal delivery. She is up to date on all vaccines. She does not walk yet but stands in place and can say a few words. The toddler drinks formula and eats a mixture of soft vegetables and pureed meals. She has no current medications. On physical exam, the vital signs include: temperature 37.0°C (98.6°F), blood pressure 95/50 mm Hg, pulse 130/min, and respiratory rate 28/min. The patient is alert and responsive. The remainder of the exam is unremarkable. Which of the following is most appropriate for this patient at this visit?
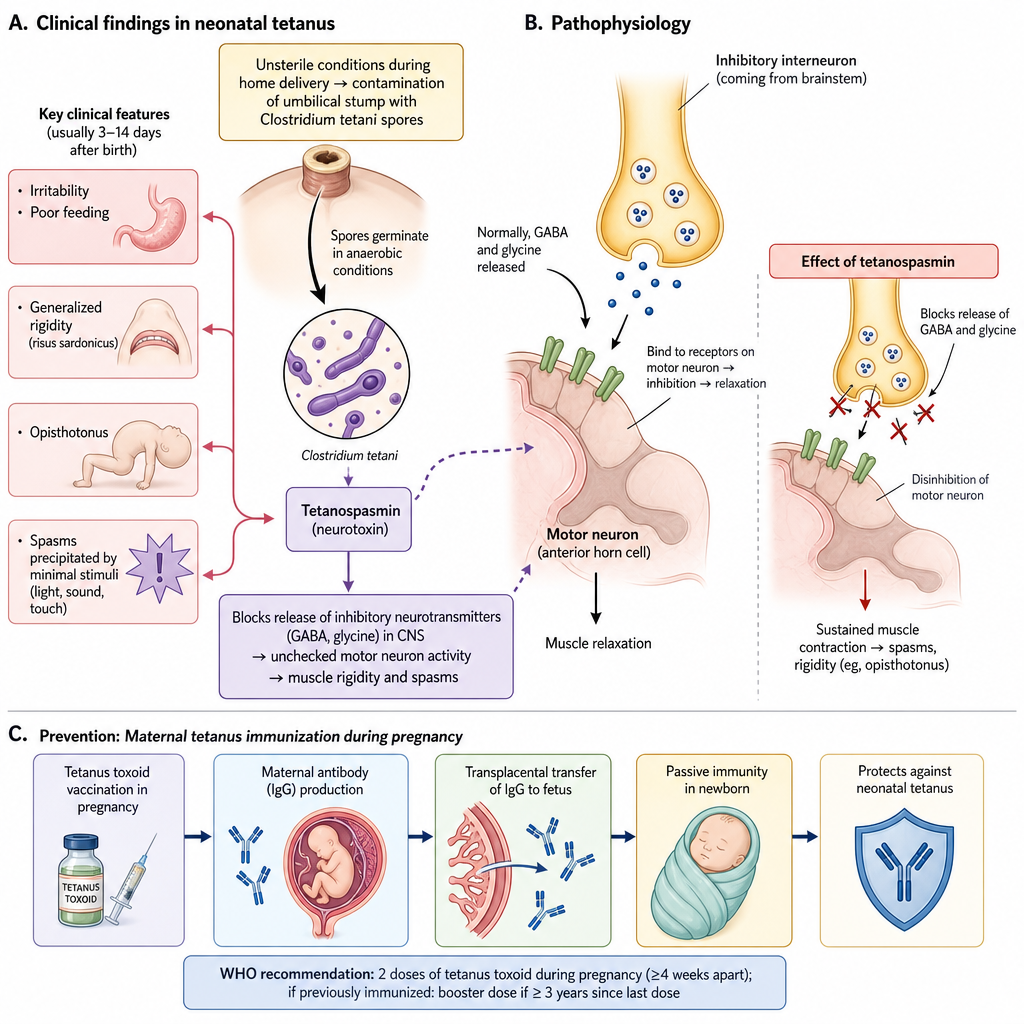
A one-week-old boy is brought to the emergency department by his mother, who recently immigrated to the United States and does not have health insurance. He was born at home, and has not received any medical care since birth. The mother states the boy has become irritable and has been feeding poorly. In the last day, she said he seems "stiff" and is having apparent muscle spasms. On your exam, you note the findings in figure A. Which of the following interventions might have prevented this disease?
A 3-year-old boy is brought to the emergency room by his mother with fever and difficulty breathing after receiving the BCG vaccine. He has never had a reaction to a vaccine before. He has a history of 2 salmonella infections over the past 2 years. He was born at 35 weeks’ gestation and spent one day in the neonatal intensive care unit. His parents' family histories are unremarkable. His temperature is 101°F (38.3°C), blood pressure is 80/55 mmHg, pulse is 135/min, and respirations are 24/min. On examination, he appears acutely ill. He has increased work of breathing with intercostal retractions. A petechial rash is noted on his trunk and extremities. A serological analysis in this patient would most likely reveal decreased levels of which of the following cytokines?
A 1-year-old immigrant girl presents to her pediatrician for a routine well-child check. She has not received any recommended vaccines since birth. She attends daycare and remains healthy despite her daily association with several other children for the past 3 months at a home daycare facility. Which of the following phenomena explains why she has not contracted any vaccine-preventable diseases such as measles, diphtheria, or pertussis?
A 7-year-old African-American boy presents to his physician with fatigue, bone and abdominal pain, and mild jaundice. The pain is dull and remitting, and the patient complains it sometimes migrates from one extremity to another. His mother reports that his jaundice and pain have occurred periodically for the past 5 years. At the time of presentation, his vital signs are as follows: the blood pressure is 80/50 mm Hg, the heart rate is 87/min, the respiratory rate is 17/min, and the temperature is 36.5°C (97.7°F). On physical examination, the patient appears to be pale with mildly icteric sclera and mucous membranes. On auscultation, there is a soft systolic ejection murmur, and palpation reveals hepatosplenomegaly. His musculoskeletal examination shows no abnormalities. Laboratory investigations show the following results: Complete blood count Erythrocytes 3.7 x 106/mm3 Hgb 11 g/dL Total leukocyte count Neutrophils Lymphocytes Eosinophils Monocytes Basophils 7,300/mm3 51% 40% 2% 7% 0 Platelet count 151,000/mm3 Chemistry Total bilirubin 3.1 mg/dL (53 µmol/L) Direct bilirubin 0.5 mg/dL (8.55 µmol/L) A peripheral blood smear shows numerous sickle-shaped red blood cells. Among other questions, the patient’s mother asks you how his condition would influence his vaccination schedule. Which of the following statements is true regarding vaccination in this patient?
Practice by Chapter
Childhood immunization schedule
Practice Questions
Catch-up vaccination protocols
Practice Questions
Vaccine contraindications and precautions
Practice Questions
Live vs inactivated vaccines
Practice Questions
Vaccine adverse events
Practice Questions
Immunocompromised host vaccination
Practice Questions
Special population considerations
Practice Questions
Vaccine storage and handling
Practice Questions
Vaccine hesitancy approaches
Practice Questions
Global vaccination programs
Practice Questions
Travel vaccines for children
Practice Questions
New and emerging vaccines
Practice Questions
Vaccination documentation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app