
Neonatal infections — MCQs

On this page
A female neonate born to a 21-year-old G2P1 had jaundice at 8 hours of life. The neonate’s red blood cell type was A+, while the mother’s RBC type was O+. The mother’s anti-A antibody titer was elevated. A screen for a fetomaternal bleed was negative. The direct Coombs test was weakly positive. The infant’s hemoglobin and total bilirubin were 10.6g/dL and 7 mg/dL, respectively. The erythrocyte glucose-6-phosphate was normal and the sickle cell test was negative. A peripheral blood smear showed normocytic normochromic RBCs, nucleated RBCs, and reticulocytes. What is the most likely diagnosis?
A 10-month-old girl is brought to the physician by her mother because of fever and irritability for the past 2 days. The mother says that the girl's diapers have smelled bad since the symptoms started. The patient has had some clear nasal secretions over the past week. Two months ago, she was brought to the emergency department for a simple febrile seizure. Otherwise, she has been healthy and her immunizations are up-to-date. She appears ill. She is at the 50th percentile for height and weight. Her temperature is 39.1°C (102.3°F), pulse is 138/min, respirations are 26/min, and blood pressure is 75/45 mm Hg. Oropharyngeal examination shows a mild postnasal drip. The remainder of the examination shows no abnormalities. Laboratory studies show: Hemoglobin 12.4 g/dL Leukocyte count 8,000/mm3 Serum Na+ 138 mEq/L K+ 4.0 mEq/L Cl- 100 mEq/L Creatinine 0.5 mg/dL Urine RBC 1–2/hpf WBC 18–20 WBCs/hpf Nitrites positive Bacteria gram-negative rods Nasal swab for respiratory syncytial virus, influenza A, and influenza B antigens is negative. Urine culture grows > 105 colony forming units (CFU)/mL of E. coli. Treatment with acetaminophen and cefixime is started. Two days later, her symptoms have improved. Which of the following is the most appropriate next step in management?
A 3580-g (7-lb 14-oz) male newborn is delivered at 36 weeks' gestation to a 26-year-old woman, gravida 2, para 1 after an uncomplicated pregnancy. His temperature is 36.7°C (98.1°F), heart rate is 96/min, and respirations are 55/min and irregular. Pulse oximetry on room air shows an oxygen saturation of 65% measured in the right hand. He sneezes and grimaces during suction of secretions from his mouth. There is some flexion movement. The trunk is pink and the extremities are blue. The cord is clamped and the newborn is dried and wrapped in a prewarmed towel. Which of the following is the most appropriate next best step in management?
A 26-year-old woman at 30 weeks 2 days of gestational age is brought into the emergency room following a seizure episode. Her medical records demonstrate poorly controlled gestational hypertension. Following administration of magnesium, she is taken to the operating room for emergency cesarean section. Her newborn daughter’s APGAR scores are 7 and 9 at 1 and 5 minutes, respectively. The newborn is subsequently taken to the NICU for further management and monitoring. Ten days following birth, the baby begins to refuse formula feedings and starts having several episodes of bloody diarrhea despite normal stool patterns previously. Her temperature is 102.2°F (39°C), blood pressure is 84/53 mmHg, pulse is 210/min, respirations are 53/min, and oxygen saturation is 96% on room air. A physical examination demonstrates a baby in mild respiratory distress and moderate abdominal distention. What do you expect to find in this patient?
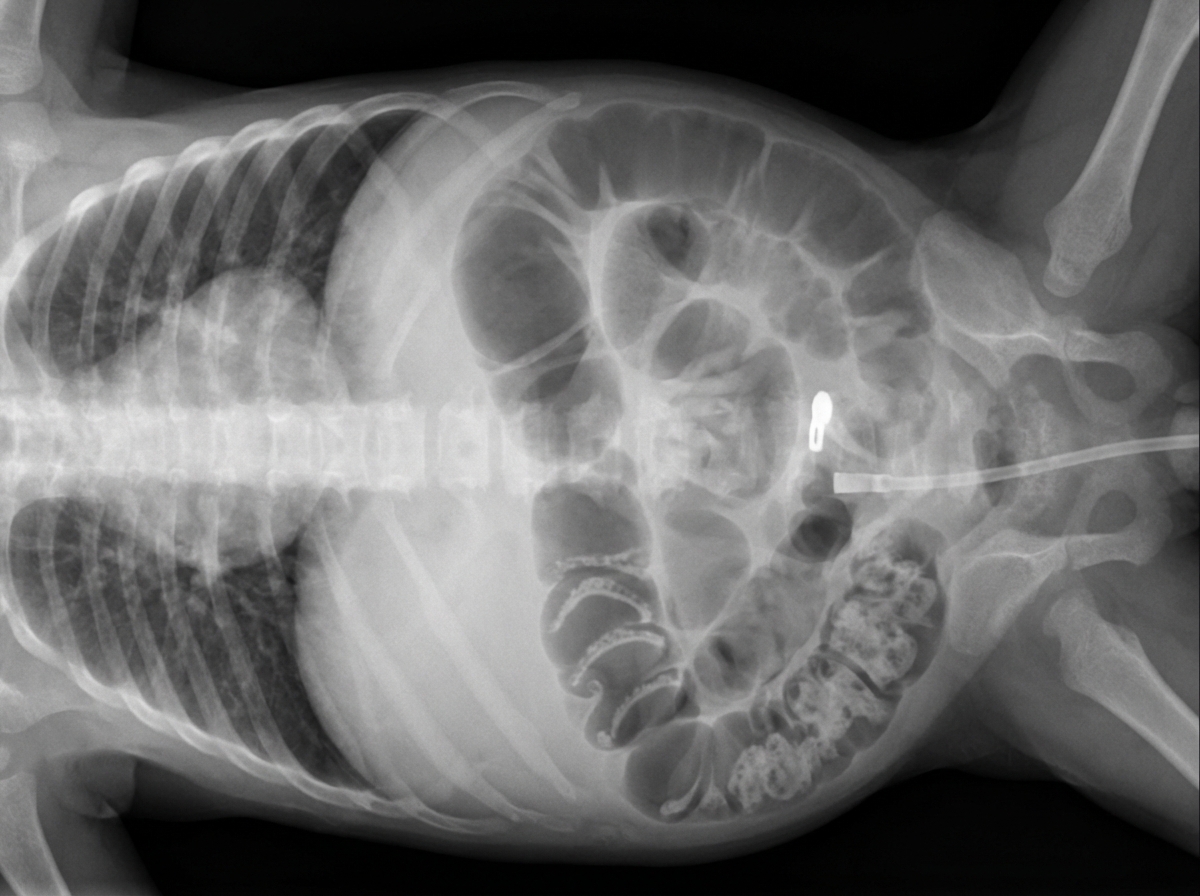
A four-week-old female is evaluated in the neonatal intensive care unit for feeding intolerance with gastric retention of formula. She was born at 25 weeks gestation to a 32-year-old gravida 1 due to preterm premature rupture of membranes at 24 weeks gestation. The patient's birth weight was 750 g (1 lb 10 oz). She required resuscitation with mechanical ventilation at the time of delivery, but she was subsequently extubated to continuous positive airway pressure (CPAP) and then weaned to nasal cannula. The patient was initially receiving both parenteral nutrition and enteral feeds through a nasogastric tube, but she is now receiving only continuous nasogastric formula feeds. Her feeds are being advanced to a target weight gain of 20-30 g per day. Her current weight is 1,350 g (2 lb 15.6 oz). The patient's temperature is 97.2°F (36.2°C), blood pressure is 72/54 mmHg, pulse is 138/min, respirations are 26/min, and SpO2 is 96% on 4L nasal cannula. On physical exam, the patient appears lethargic. Her abdomen is soft and markedly distended. Digital rectal exam reveals stool streaked with blood in the rectal vault. Which of the following abdominal radiographs would most likely be seen in this patient?
A 3-day-old boy develops several episodes of complete body shaking while at the hospital. The episodes last for about 10–20 seconds. He has not had fever or trauma. He was born at 40 weeks' gestation and has been healthy. The mother did not follow-up with her gynecologist during her pregnancy on a regular basis. There is no family history of serious illness. The patient appears irritable. Vital signs are within normal limits. Physical examination shows reddening of the face. Peripheral venous studies show a hematocrit of 68%. Neuroimaging of the head shows several cerebral infarctions. Which of the following is the most likely cause of this patient's findings?
A previously healthy 6-month-old boy is brought to the emergency department because of irritability and poor feeding for 6 days. He has also not had a bowel movement in 9 days and has been crying less than usual. He is bottle fed with formula and his mother has been weaning him with mashed bananas mixed with honey for the past 3 weeks. His immunizations are up-to-date. He appears weak and lethargic. He is at the 50th percentile for length and 75th percentile for weight. Vital signs are within normal limits. Examination shows dry mucous membranes and delayed skin turgor. There is poor muscle tone and weak head control. Neurological examination shows ptosis of the right eye. Which of the following is the most appropriate initial treatment?
A 1-minute-old newborn is being examined by the pediatric nurse. The nurse auscultates the heart and determines that the heart rate is 89/min. The respirations are spontaneous and regular. The chest and abdomen are both pink while the tips of the fingers and toes are blue. When the newborn’s foot is slapped the face grimaces and he cries loud and strong. When the arms are extended by the nurse they flex back quickly. What is this patient’s Apgar score?
A 7-year-old boy is brought to a pediatric clinic by his mother because he had difficulty swallowing for 4 days. He was diagnosed with asthma 3 months ago and has been using an inhaled corticosteroid as directed by the pediatrician. The child does not have a fever or a cough and is not short of breath. He denies pain during swallowing. His vital signs include: temperature 35.8℃ (96.5℉), respiratory rate 14/min, blood pressure 90/40 mm Hg, and pulse 80/min. The oral examination reveals a slightly raised white lesion over his tongue (as shown in the provided photograph) and oropharynx. What is the most likely diagnosis?

A 4-day-old male newborn is brought to the physician because of increasing yellowish discoloration of his skin for 2 days. He was born at 38 weeks' gestation and weighed 2466 g (5 lb 7 oz); he currently weighs 2198 g (4 lb 14 oz). Pregnancy was complicated by pregnancy-induced hypertension. The mother says he breastfeeds every 3 hours and has 3 wet diapers per day. His temperature is 37°C (98.6°F), pulse is 165/min, and respirations are 53/min. Examination shows jaundice and scleral icterus. The anterior fontanelle is mildly sunken. The abdomen is soft and nontender; there is no organomegaly. The remainder of the examination shows no abnormalities. Laboratory studies show: Hematocrit 58% Serum Bilirubin _ Total 20 mg/dL _ Conjugated 0.8 mg/dL Which of the following is the most likely cause of these findings?
Practice by Chapter
Early-onset sepsis
Practice Questions
Late-onset sepsis
Practice Questions
Group B streptococcal disease
Practice Questions
Neonatal meningitis
Practice Questions
Congenital TORCH infections
Practice Questions
Neonatal HSV
Practice Questions
Neonatal candidiasis
Practice Questions
Necrotizing enterocolitis
Practice Questions
Omphalitis
Practice Questions
Nursery outbreaks
Practice Questions
Antibiotic stewardship in NICU
Practice Questions
Diagnostic approach to neonatal sepsis
Practice Questions
Maternal factors and neonatal infection risk
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app