
Maternal factors and neonatal infection risk — MCQs

A 6-year-old boy and his parents present to the emergency department with high-grade fever, headache, and projectile vomiting. The boy was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. Past medical history is noncontributory. He has had no sick contacts at school or at home. The family has not traveled out of the area recently. He likes school and playing videogames with his younger brother. Today, his blood pressure is 115/76 mm Hg, heart rate is 110/min, respiratory rate is 22/min, and temperature is 38.4°C (101.2°F). On physical exam, the child is disoriented. Kernig’s sign is positive. A head CT was performed followed by a lumbar puncture. Several aliquots of CSF were distributed throughout the lab. Cytology showed high counts of polymorphs, biochemistry showed low glucose and elevated protein levels, and a gram smear shows gram-positive lanceolate-shaped cocci alone and in pairs. A smear is prepared on blood agar in an aerobic environment and grows mucoid colonies with clearly defined edges and alpha hemolysis. On later evaluation they develop a ‘draughtsman’ appearance. Which one of the following is the most likely pathogen?
A 6-day-old newborn is brought to the emergency department by his mother due to a high fever that started last night. His mother says that he was born via an uneventful vaginal delivery at home at 38 weeks gestation and was doing fine up until yesterday when he became disinterested in breastfeeding and spit up several times. His temperature is 39.5°C (103.1°F), pulse is 155/min, respirations are 45/min, and O2 sats are 92% on room air. He is lethargic and minimally responsive to stimuli. While on his back, his head is quickly lifted towards his chest which causes his legs to flex. The mother had only a few prenatal care visits and none at the end of the pregnancy. What is the most likely source of this patients infection?
A 28-year-old female in the 2nd trimester of pregnancy is diagnosed with primary Toxoplasma gondii infection. Her physician fears that the fetus may be infected in utero. Which of the following are associated with T. gondii infection in neonates?
A 27-year-old woman, gravida 2, para 1, at 36 weeks' gestation comes to the physician for a prenatal visit. She feels well. Fetal movements are adequate. This is her 7th prenatal visit. She had an ultrasound scan performed 1 month ago that showed a live intrauterine pregnancy consistent with a 32-week gestation with no anomalies. She had a Pap smear performed 1 year ago, which was normal. Vital signs are within normal limits. Pelvic examination shows a uterus consistent in size with a 36-week gestation. Her blood group and type is A negative. Which of the following is the most appropriate next step in management?
A 28-year-old primigravid woman at 36 weeks' gestation comes to the emergency department because of worsening pelvic pain for 2 hours. Three days ago, she had a burning sensation with urination that resolved spontaneously. She has nausea and has vomited fluid twice on her way to the hospital. She appears ill. Her temperature is 39.7°C (103.5°F), pulse is 125/min, respirations are 33/min, and blood pressure is 130/70 mm Hg. Abdominal examination shows diffuse tenderness. No contractions are felt. Speculum examination shows pooling of nonbloody, malodorous fluid in the vaginal vault. The cervix is not effaced or dilated. Laboratory studies show a hemoglobin concentration of 14 g/dL, a leukocyte count of 16,000/mm3, and a platelet count of 250,000/mm3. Fetal heart rate is 148/min and reactive with no decelerations. Which of the following is the most appropriate next step in management?
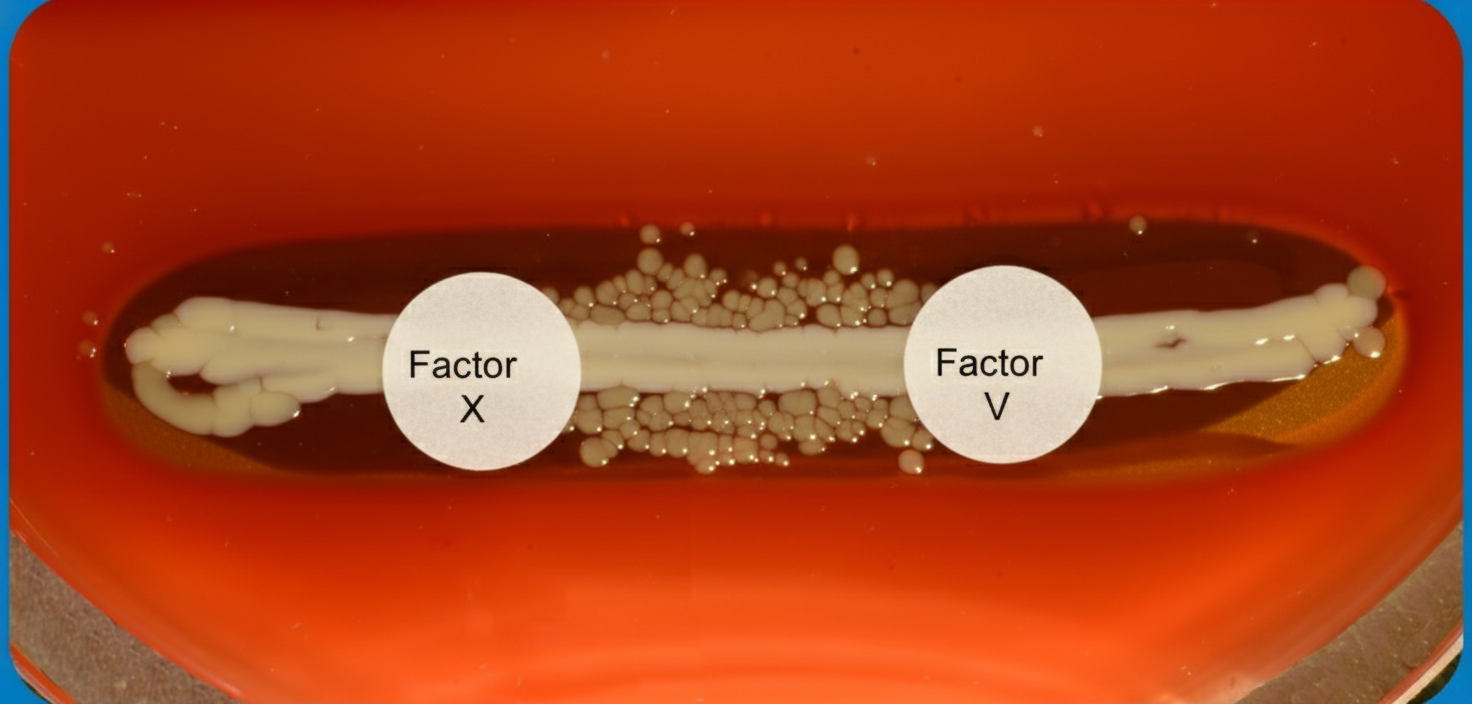
A 6-month old child is brought to the ER by parents for one day of fever, decreased feeding, and lethargy. They report that neither she nor her siblings are immunized due to their concerns about vaccinations. On exam, the infant is toxic-appearing. Antibiotics are started and lumbar puncture reveals bacterial meningitis caused by a gram-negative, encapsulated organism that requires chocolate agar and the two factors shown in Image A for growth. Which organism does this best describe?
A male neonate is being examined by a pediatrician. His mother informs the doctor that she had a mild fever with rash, muscle pain, and swollen and tender lymph nodes during the second month of gestation. The boy was born at 39 weeks gestation via spontaneous vaginal delivery with no prenatal care. On physical examination, the neonate has normal vital signs. Retinal examination reveals the findings shown in the image. Which of the following congenital heart defects is most likely to be present in this neonate?

A mother delivers in a rural area under the guidance of a skilled care attendant. Which of the following statements is incorrect regarding the care provided by the skilled care attendant at birth?
A 9-month-old boy is brought to the physician because of abnormal crawling and inability to sit without support. A 2nd-trimester urinary tract infection that required antibiotic use and a spontaneous preterm birth via vaginal delivery at 36 weeks’ gestation both complicated the mother’s pregnancy. Physical examination shows a scissoring posture of the legs when the child is suspended by the axillae. Examination of the lower extremities shows brisk tendon reflexes, ankle clonus, and upward plantar reflexes bilaterally. When encouraged by his mother, the infant crawls forward by using normal reciprocal movements of his arms, while his legs drag behind. A brain MRI shows scarring and atrophy in the white matter around the ventricles with ventricular enlargement. Which of the following is most likely associated with the findings in this child?
A 34-year-old man with a 2-year history of rheumatoid arthritis is being evaluated on a follow-up visit. He is currently on methotrexate and celecoxib for pain management and has shown a good response until now. However, on this visit, he mentions that the morning stiffness has been getting progressively worse. On physical examination, both his wrists are erythematous and swollen, nodules on his elbows are also noted. Rheumatoid factor is 30 (normal reference values: < 15 IU/mL), ESR is 50 mm/h, anti-citrullinated protein antibodies is 55 (normal reference values: < 20). What is the next best step in the management of this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app