
Milestones — MCQs

On this page
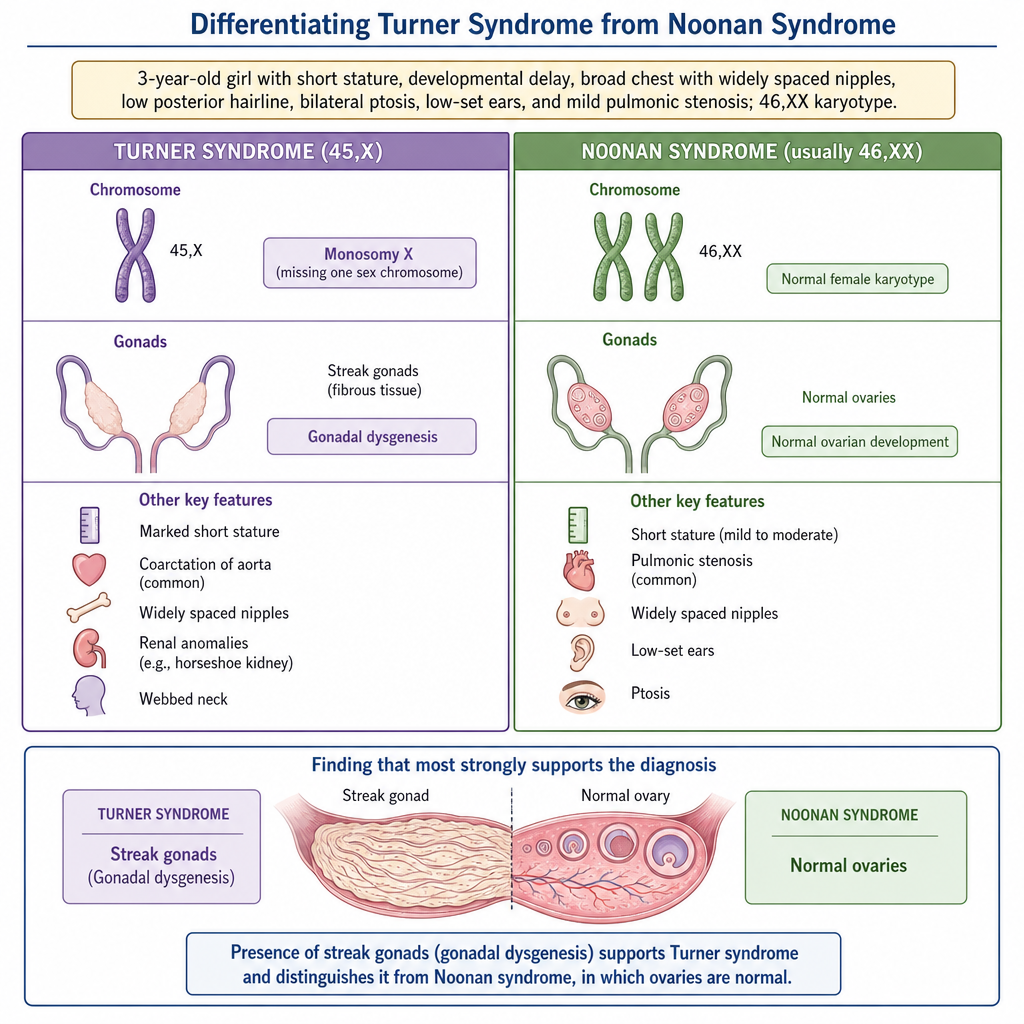
A 3-year-old girl is referred for evaluation of short stature and developmental concerns. On examination, she has a broad chest with widely spaced nipples, low posterior hairline, bilateral ptosis, low-set ears, and mild pulmonic stenosis on echocardiogram. Her chromosomal analysis reveals a 46,XX karyotype. Which of the following additional findings would most strongly support the unifying diagnosis in this child compared with the most phenotypically similar condition in the differential?
A 3-year-old boy is brought to the office by his mother because of a large head contusion and altered mental status. At first, the mother says her son got injured when a “pot fell from a shelf onto his head.” Later, she changes the story and says that he hit his head after “tripping over a football.” Physical examination shows cracks in the suture lines of the skull, and there is a flattened appearance to the bone. The patient’s father arrives to inquire on how his son is “recovering from his fall down the stairs.” Upon request to interview the patient alone, the parents refuse, complaining loudly about the request. Which of the following is the most likely diagnosis in this patient?
A 4-month-old boy is brought to the physician for a well-child examination. He was born at 39 weeks gestation via spontaneous vaginal delivery and is exclusively breastfed. He weighed 3,400 g (7 lb 8 oz) at birth. At the physician's office, he appears well. His pulse is 146/min, the respirations are 39/min, and the blood pressure is 78/44 mm Hg. He weighs 7.5 kg (16 lb 9 oz) and measures 65 cm (25.6 in) in length. The remainder of the physical examination is normal. Which of the following developmental milestones has this patient most likely met?
A 6-month-old girl presents to an outpatient office for a routine physical. She can sit momentarily propped on her hands, babbles with consonants, and transfers objects hand to hand. The pediatrician assures the parents that their daughter has reached appropriate developmental milestones. Which additional milestone would be expected at this stage in development?
A 4-year-old boy is brought to the physician by his parents for bedwetting. He went 3 months without wetting the bed but then started again 6 weeks ago. He has been wetting the bed about 1–2 times per week. He has not had daytime urinary incontinence or dysuria. His teachers report that he is attentive in preschool and plays well with his peers. He is able to name 5 colors, follow three-step commands, and recite his address. He can do a somersault, use scissors, and copy a square. Physical examination shows no abnormalities. Which of the following is the most appropriate next step in management?
Practice by Chapter
Gross motor milestones
Practice Questions
Fine motor milestones
Practice Questions
Language development
Practice Questions
Social-emotional development
Practice Questions
Cognitive development
Practice Questions
Denver Developmental Screening Test
Practice Questions
Red flags for developmental delay
Practice Questions
Developmental surveillance
Practice Questions
Delayed milestones evaluation
Practice Questions
Early intervention services
Practice Questions
Milestone variations in preterm infants
Practice Questions
Cultural influences on development
Practice Questions
Developmental regression causes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app