
Kawasaki disease — MCQs

On this page
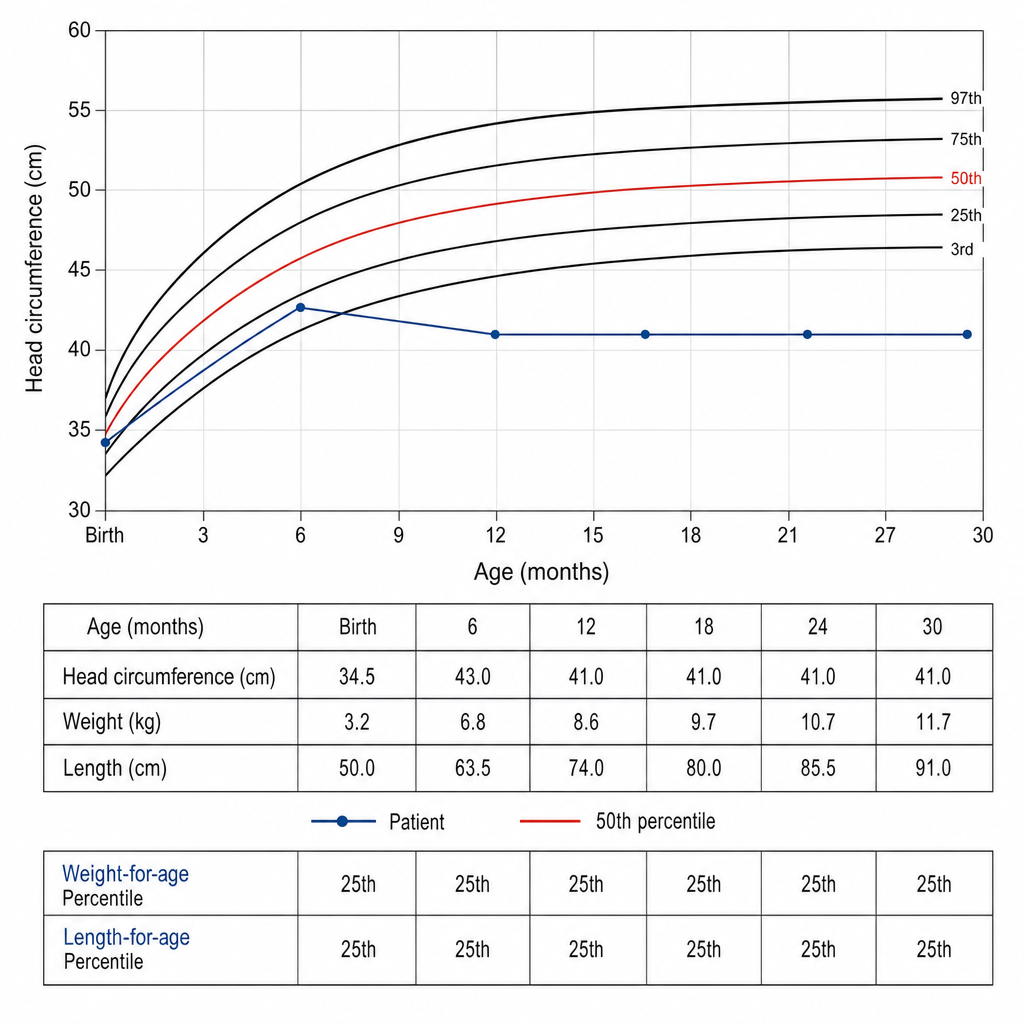
A girl is evaluated at 30 months of age. Her head circumference has crossed from the 50th percentile at birth to below the 3rd percentile at 12 months and has remained there. Her weight and length are tracking along the 25th percentile. She was born at term without perinatal complications. She was noted to have normal social smiling and babbling at 6 months, but her mother reports a period of apparent developmental regression between 12 and 18 months during which she lost purposeful hand use and began repetitive hand-wringing movements. Which genetic mechanism most likely accounts for this clinical picture?
A 4-year-old boy is brought to the physician by his parents because of fever and mild abdominal pain for 7 days. His parents report that he developed a rash 2 days ago. He has had no diarrhea or vomiting. Four weeks ago, he returned from a camping trip to Colorado with his family. His immunization records are unavailable. His temperature is 39.4°C (102.9°F), pulse is 111/min, respirations are 27/min, and blood pressure is 96/65 mm Hg. Examination shows bilateral conjunctival injections and fissures on his lower lips. The pharynx is erythematous. There is tender cervical lymphadenopathy. The hands and feet appear edematous. A macular morbilliform rash is present over the trunk. Bilateral knee joints are swollen and tender; range of motion is limited by pain. Which of the following is the most appropriate treatment for this patient's condition?
A 4-year-old boy is brought to a pediatrician by his parents with a history of fever for the last 5 days and irritability, decreased appetite, vomiting, and swelling of the hands and feet for the last 3 days. The patient’s mother mentions that he has been taking antibiotics and antipyretics prescribed by another physician for the last 3 days, but there has been no improvement His temperature is 39.4°C (103.0°F), pulse is 128/min, respiratory rate is 24/min, and blood pressure is 96/64 mm Hg. On physical examination, there is significant edema of the hands and feet bilaterally. There is a 2.5 cm diameter freely moveable, nontender cervical lymph node is palpable on the right side. A strawberry tongue and perianal erythema are noted. Conjunctival injection is present bilaterally. Laboratory findings reveal mild anemia and a leukocytosis with a left-shift. Erythrocyte sedimentation rate (ESR) and serum C-reactive protein (CRP) are increased. If not treated appropriately, this patient is at increased risk of developing which of the following complications?
A 5-year-old girl presents with a rash and a persistent fever of 41.0°C (105.8°F), not relieved by Tylenol. The patient's mother says that her symptoms started 5 days ago and have not improved. The rash started on her trunk and now is present everywhere including the palms and soles. Her birth history is normal. Her pulse is 120/min and respiratory rate is 22/min. On physical examination, the patient is agitated and ill-appearing. There is significant swelling of the distal upper and lower extremities bilaterally. The pharynx is hyperemic (see image). Generalized edema with palpable cervical lymphadenopathy is noted. Muscle tone is normal. Remainder of exam is unremarkable. Laboratory findings are significant for the following: Laboratory test Hb 9 g/dL RBC 3.3/mm3 Neutrophilic leukocytosis 28,000/mm3 Normal platelet count 200,000/mm3 Serum ɣ-GT increased Hyperbilirubinemia 2.98 mg/dL AST and ALT are normal, but there is markedly increased serum CRP. Which of the following is the most likely diagnosis in this patient?

A previously healthy 4-year-old boy is brought to the physician by his parents because he has had a fever, diffuse joint pain, and a rash on his abdomen for the past week. Acetaminophen did not improve his symptoms. He emigrated from China with his family 2 years ago. He attends daycare. His immunization records are not available. His temperature is 38.5°C (101.3°F), pulse is 125/min, and blood pressure is 100/60 mm Hg. Examination shows polymorphous truncal rash. The eyes are pink with no exudate. The tongue is shiny and red, and the lips are cracked. The hands and feet are red and swollen. There is right-sided anterior cervical lymphadenopathy. Which of the following is the most appropriate next step in management?
Practice by Chapter
Diagnostic criteria and clinical features
Practice Questions
Atypical Kawasaki presentation
Practice Questions
Laboratory findings
Practice Questions
Cardiac complications and evaluation
Practice Questions
Acute phase management
Practice Questions
IVIG resistance
Practice Questions
Coronary artery aneurysms
Practice Questions
Long-term cardiac follow-up
Practice Questions
Differential diagnosis
Practice Questions
Recurrence risk
Practice Questions
Pathophysiology theories
Practice Questions
Age-specific considerations
Practice Questions
Long-term outcomes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app