
Infectious Disease — MCQs

On this page
A 7-year-old boy is brought into the emergency department after he was found at home by his mother possibly drinking a drain cleaning solution from under the sink. The child consumed an unknown amount and appears generally well. The child has an unremarkable past medical history and is not currently taking any medications. Physical exam reveals a normal cardiopulmonary and abdominal exam. Neurological exam is within normal limits and the patient is cooperative and scared. The parents state that the ingestion happened less than an hour ago. Which of the following is the best next step in management?
A 5-year-old boy is brought to the emergency department by his grandmother because of difficulty breathing. Over the past two hours, the grandmother has noticed his voice getting progressively hoarser and occasionally muffled, with persistent drooling. He has not had a cough. The child recently immigrated from Africa, and the grandmother is unsure if his immunizations are up-to-date. He appears uncomfortable and is sitting up and leaning forward with his chin hyperextended. His temperature is 39.5°C (103.1°F), pulse is 110/min, and blood pressure is 90/70 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 95%. Pulmonary examination shows inspiratory stridor and scattered rhonchi throughout both lung fields, along with poor air movement. Which of the following is the most appropriate next step in management?
A 10-year-old boy with bronchial asthma is brought to the physician by his mother because of a generalized rash for 2 days. He has also had a fever and sore throat for 4 days. The rash involves his whole body and is not pruritic. His only medication is a fluticasone-salmeterol combination inhaler. He has not received any routine childhood vaccinations. His temperature is 38.5°C (101.3°F) and pulse is 102/min. Examination shows dry mucous membranes and a flushed face except around his mouth. A diffuse, maculopapular, erythematous rash that blanches with pressure is seen over the trunk along with a confluence of petechiae in the axilla. Oropharyngeal examination shows pharyngeal erythema with a red beefy tongue. His hemoglobin is 13.5 mg/dL, leukocyte count is 11,200/mm3 (75% segmented neutrophils, 22% lymphocytes), and platelet count is 220,000/mm3. The clinical presentation is consistent with scarlet fever. Which of the following is the most likely sequela of this condition?
A 12-year-old girl is brought to the emergency department by her parents due to severe shortness of breath that started 20 minutes ago. She has a history of asthma and her current treatment regime includes a beta-agonist inhaler as well as a medium-dose corticosteroid inhaler. Her mother tells the physician that her daughter was playing outside with her friends when she suddenly started experiencing difficulty breathing and used her inhaler without improvement. On examination, she is struggling to breathe and with subcostal and intercostal retractions. She is leaning forward, and gasping for air and refuses to lie down on the examination table. Her blood pressure is 130/92 mm Hg, the respirations are 27/min, the pulse is 110/min and O2 saturation is 87%. There is prominent expiratory wheezes in all lung fields. The patient is put on a nonrebreather mask with 100% oxygen. An arterial blood gas is collected and sent for analysis. Which of the following is the most appropriate next step in the management of this patient?
A 15-month-old girl is brought to the physician because of the sudden appearance of a rash on her trunk that started 6 hours ago and subsequently spread to her extremities. Four days ago, she was taken to the emergency department because of a high fever and vomiting. She was treated with acetaminophen and discharged the next day. The fever persisted for several days and abated just prior to appearance of the rash. Physical examination shows a rose-colored, blanching, maculopapular rash, and postauricular lymphadenopathy. Which of the following is the most likely diagnosis?
A 9-year-old boy presents to the emergency department with a 12-hour history of severe vomiting and increased sleepiness. He experienced high fever and muscle pain about 5 days prior to presentation, and his parents gave him aspirin to control the fever at that time. On presentation, he is found to be afebrile though he is still somnolent and difficult to arouse. Physical exam reveals hepatomegaly and laboratory testing shows the following results: Alanine aminotransferase: 85 U/L Aspartate aminotransferase: 78 U/L Which of the following is the most likely cause of this patient's neurologic changes?
A previously healthy 10-year-old boy is brought to the emergency department 15 minutes after he had a seizure. His mother reports that he complained of sudden nausea and seeing “shiny lights,” after which the corner of his mouth and then his face began twitching. Next, he let out a loud scream, dropped to the floor unconscious, and began to jerk his arms and legs as well for about two minutes. On the way to the hospital, the boy regained consciousness, but was confused and could not speak clearly for about five minutes. He had a fever and sore throat one week ago which improved after treatment with acetaminophen. He appears lethargic and cannot recall what happened during the episode. His vital signs are within normal limits. He is oriented to time, place, and person. Deep tendon reflexes are 2+ bilaterally. There is muscular pain at attempts to elicit deep tendon reflexes. Physical and neurologic examinations show no other abnormalities. Which of the following is the most likely diagnosis?
A 16-month-old male patient, with no significant past medical history, is brought into the emergency department for the second time in 5 days with tachypnea, expiratory wheezes and hypoxia. The patient presented to the emergency department initially due to rhinorrhea, fever and cough. He was treated with nasal suctioning and discharged home. The mother states that, over the past 5 days, the patient has started breathing faster with chest retractions. His vital signs are significant for a temperature of 100.7 F, respiratory rate of 45 and oxygen saturation of 90%. What is the most appropriate treatment for this patient?
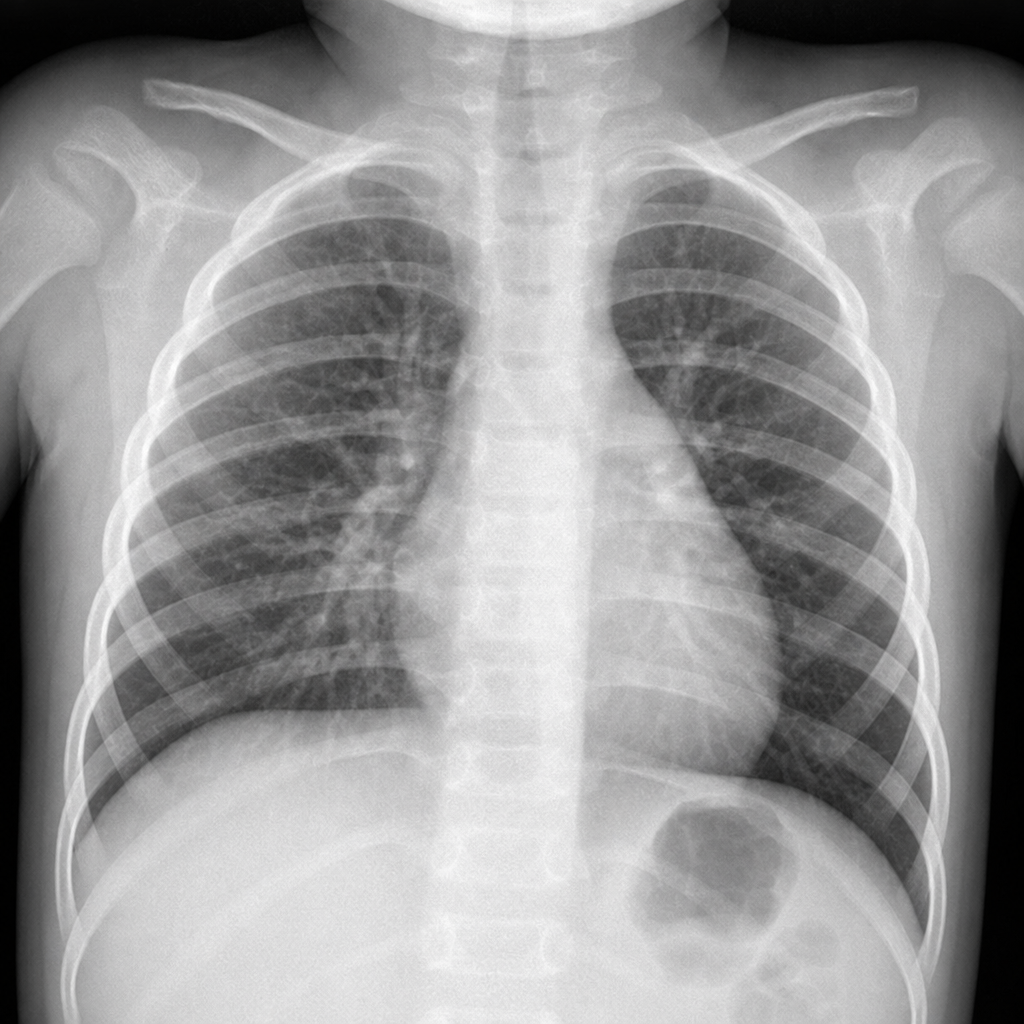
A 3-year-old boy is brought to his pediatrician’s office because of prolonged ear pulling and discomfort. The condition started a week ago and his parents are concerned that he has developed another ear infection. He has had multiple minor respiratory tract infections with productive cough and ear infections over the last year; he has also been hospitalized once with community-acquired pneumonia. During his last ear infection, there was some discussion of myringotomy. The boy was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. Today, the vital signs include: temperature 39.0°C (102.0°F), blood pressure 100/65 mm Hg, heart rate 110/min, and respiratory rate 30/min. His left ear is tender and appears red and irritated. Examination with an otoscope reveals a swollen canal and a bulging tympanic membrane. A review of previous medical records reveals the following chest X-ray taken 2 months ago. What is the underlying cause of his recurrent infections?
A 10-month-old girl is brought to the clinic by her mother with skin lesions on her chest. The mother says that she noticed the lesions 24 hours ago and that they have not improved. The patient has no significant past medical history. She was born at term by spontaneous transvaginal delivery with no complications, is in the 90th percentile on her growth curve, and has met all developmental milestones. Upon physical examination, several skin-colored umbilicated papules are visible. Which of the following is the most appropriate treatment of this patient's likely diagnosis?
Practice by Chapter
Common childhood exanthems
Practice Questions
Pediatric respiratory infections
Practice Questions
Pediatric gastrointestinal infections
Practice Questions
Urinary tract infections in children
Practice Questions
Bone and joint infections
Practice Questions
Central nervous system infections
Practice Questions
Pediatric tuberculosis
Practice Questions
Pediatric HIV
Practice Questions
Recurrent infections evaluation
Practice Questions
Fever of unknown origin approach
Practice Questions
Emerging infectious diseases in children
Practice Questions
Post-infectious immune complications
Practice Questions
Antimicrobial resistance in pediatrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app