
Infectious Disease — MCQs

On this page
A 16-year-old girl is brought to the physician for recurrent episodes of shortness of breath, nonproductive cough, and chest tightness for 3 months. These episodes occur especially while playing sports and resolve spontaneously with rest. She appears healthy. Her pulse is 63/min, respirations are 15/min, and blood pressure is 102/70 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 98%. Physical examination shows no abnormalities. An x-ray of the chest shows no abnormalities. Spirometry shows a FEV1:FVC ratio of 85% and a FEV1of 85% of predicted. Which of the following is the most appropriate next step in management?
A 4-year-old boy is brought to the emergency department because of fever, nausea, and headache for 1 day. His temperature is 39.7°C (103.5°F). Examination shows involuntary flexion of the knees and hips when the neck is flexed. A lumbar puncture is performed and cerebrospinal fluid (CSF) analysis shows numerous segmented neutrophils and a decreased glucose concentration. Gram stain of the CSF shows gram-negative diplococci. This patient is at increased risk for which of the following complications?
A 6-year-old male is brought to the pediatrician by his mother because she is concerned about his breathing. She states that every once in a while he seems to have bouts of coughing but doesn't have any significant difficulty breathing. She demands that the pediatrician begin treatment with albuterol as she is convinced that her child has asthma. The pediatrician, not fully convinced, states that he will run a test that will help to rule out asthma as a diagnosis. To which of the following tests is the pediatrician referring?
A 3-year-old boy is brought to the emergency department by his mother for abdominal pain. She states that he has refused to eat and keeps clutching his stomach saying “ow.” She reports that he has not had any vomiting or diarrhea. She says that he has not had a bowel movement in 3 days. The family recently moved from Namibia and has not established care. He has no known medical conditions and takes no medications. The mother says there is a family history of a “blood illness.” On physical examination, there is mild distension with tenderness in the bilateral lower quadrants without organomegaly. An ultrasound of the abdomen reveals 2 gallstones without gallbladder wall thickening or ductal dilation and a negative Murphy sign. An abdominal radiograph shows moderate stool burden in the large bowel and rectum. Labs are obtained, as below: Hemoglobin: 9 g/dL Platelet count: 300,000/mm^3 Mean corpuscular volume (MCV): 85 µm^3 Reticulocyte count: 5% Lactate dehydrogenase (LDH): 532 U/L Leukocyte count: 11/mm^3 Serum iron: 140 mcg/dL Transferrin saturation: 31% (normal range 20-50%) Total iron binding capacity (TIBC): 400 mcg/dL (normal range 240 to 450 mcg/dL) A hemoglobin electrophoresis shows hemoglobin S, increased levels of hemoglobin F, and no hemoglobin A. The results are discussed with the patient’s mother including recommendations for increasing fiber in the patient’s diet and starting hydroxyurea. Which of the following should also be part of management for the patient’s condition?
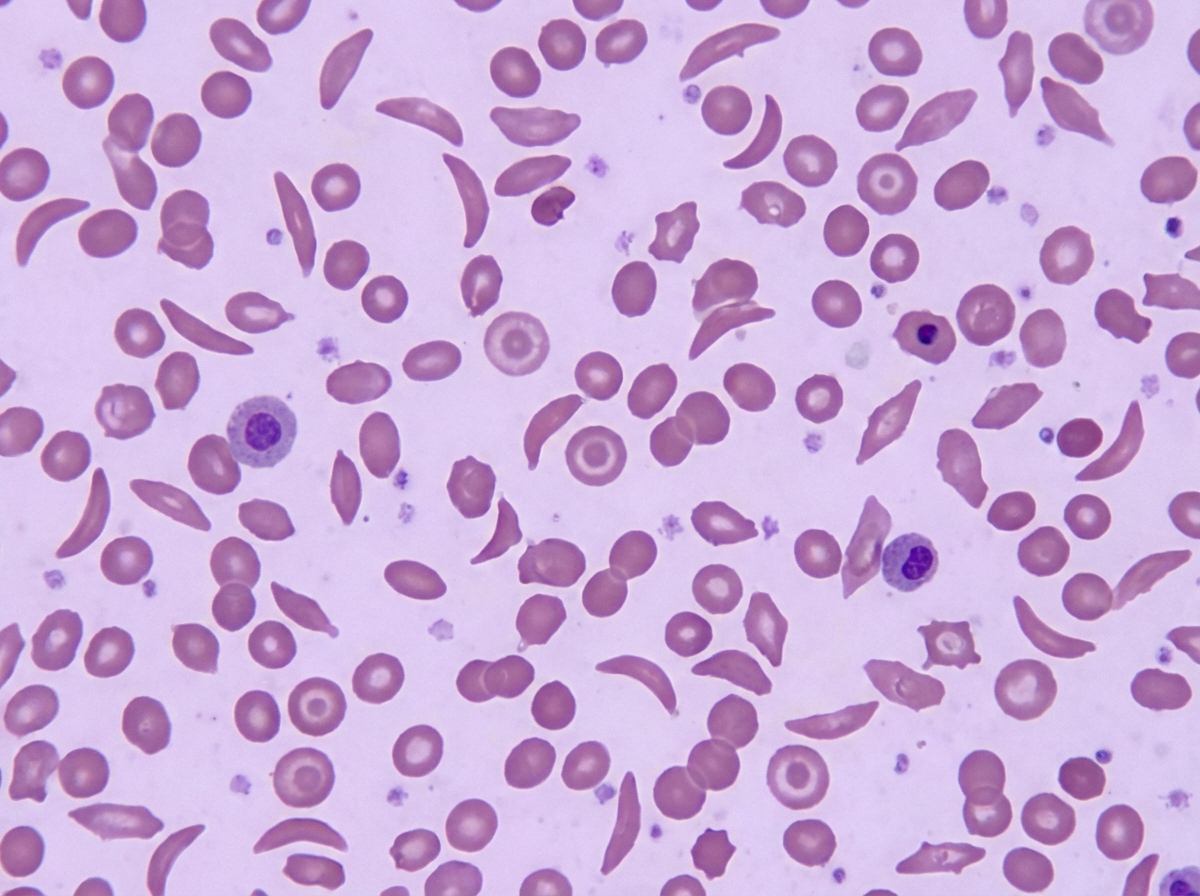
A 2-year-old girl is brought to the emergency department because of bilateral hand pain and swelling. Her parents say the pain began 1 week ago and has gotten progressively worse. The patient appears to be in distress. Her temperature is 38.5°C (101.4°F), pulse is 130/min, and respirations are 25/min. The dorsum of her hands and fingers are erythematous, swollen, warm, and tender to palpation. Her hemoglobin concentration is 9.1 g/dL and leukocyte count is 8,000/mm3. A peripheral blood smear is shown. Which of the following interventions is most appropriate to prevent a recurrence of this patient's symptoms?
A 5-year-old boy with a history of severe allergies and recurrent sinusitis presents with foul-smelling, fatty diarrhea. He is at the 50th percentile for height and weight. The boy's mother reports that he has had several such episodes of diarrhea over the years. He does not have any known history of fungal infections or severe viral infections. Which of the following is the most likely underlying cause of this boy's presentation?
A 4-year-old boy presents to the emergency department after his parents found him drinking blue liquid out of an unlabeled bottle in the garage. They have no idea what was in the bottle and are concerned for his health. They have brought the bottle with them to the emergency department. The child's past medical history is not remarkable, and he is currently not taking any medications. The patient's vitals are within normal limits for his age. Physical exam reveals a crying child who is drooling. A radiograph is performed, and the child's vitals are closely monitored. It is determined that the blue liquid is a strong alkali. Which of the following is the best next step in management?
A 3-year-old boy presents with fever, generalized fatigue, nausea, and progressive anemia. The patient’s mother says his condition was normal until one week ago when he started having flu-like symptoms such as fever, general fatigue, and abdominal discomfort. Past medical experience is significant for sickle cell disease, diagnosed 2 years ago. His vital signs include: blood pressure 98/50 mm Hg, pulse 120/min, temperature 39.0℃ (102.0℉). On physical examination, the patient is crying excessively and his skin and the conjunctivae look pale. Splenomegaly is noted. There is no skin rash nor lymphadenopathy. Laboratory findings are significant for the following: Total WBC count 22,000/mm3 Neutrophils 35% Lymphocytes 44% Atypical lymphocytes 9% Monocytes 12% RBC 1. 6 million/mm3 Hb 5.4 g/dL Hct 14.4% MCV 86 fL MCHC 37.5% Reticulocytes 0.1% A peripheral blood smear shows sickle cells. A direct and indirect Coombs test is negative. Which of the following is the most likely cause of this patient’s most recent symptoms?
A 7-year-old girl is brought to the physician because of generalized fatigue and dark urine for 1 week. Four weeks ago, she was treated with topical mupirocin for a skin infection. Her 5-year-old brother has steroid-resistant nephrotic syndrome. Her temperature is 37°C (98.6°F), pulse is 90/min, respirations are 14/min, and blood pressure is 132/89 mm Hg. Examination shows periorbital and 1+ pretibial edema bilaterally. The remainder of the examination shows no abnormalities. Laboratory studies show: Hemoglobin 12.9 g/dL Leukocyte count 7,200/mm3 Platelet count 230,000/mm3 Serum Urea nitrogen 32 mg/dL Creatinine 1.8 mg/dL Urine Blood 2+ Protein 2+ Glucose negative RBC 12–14/hpf with dysmorphic features RBC casts numerous Which of the following is the most likely cause of these findings?
A 3-month-old boy presents to his pediatrician with persistent diarrhea, oral candidiasis, and signs and symptoms of respiratory syncytial virus (RSV) pneumonia. He is very lean with weight in the 10th percentile. His blood pressure is 105/64 mm Hg and heart rate is 84/min. He is being evaluated for an immunodeficiency. Laboratory results for HIV are negative by polymerase chain reaction (PCR). Which of the following is the most likely cause of this child’s presentation?
Practice by Chapter
Common childhood exanthems
Practice Questions
Pediatric respiratory infections
Practice Questions
Pediatric gastrointestinal infections
Practice Questions
Urinary tract infections in children
Practice Questions
Bone and joint infections
Practice Questions
Central nervous system infections
Practice Questions
Pediatric tuberculosis
Practice Questions
Pediatric HIV
Practice Questions
Recurrent infections evaluation
Practice Questions
Fever of unknown origin approach
Practice Questions
Emerging infectious diseases in children
Practice Questions
Post-infectious immune complications
Practice Questions
Antimicrobial resistance in pediatrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app