
Infectious Disease — MCQs

On this page
A 6-year-old girl is brought to a clinic with complaints of fever and sore throat for 2 days. This morning, she developed a rash on the trunk and flexural areas which is spreading outward, with facial flushing and circumoral pallor. The teachers in her school report that none of her classmates has similar symptoms. She has a normal birth history. On physical examination, the child looks healthy. The heart rate is 90/min, respiratory rate is 20/min, temperature is 39.0°C (102.2°F), and blood pressure is 90/50 mm Hg. An oropharyngeal examination reveals circumoral pallor with a red tongue, as shown in the photograph below. The chest and cardiac examinations are within normal limits. No hepatosplenomegaly is noted. What is the most likely diagnosis?

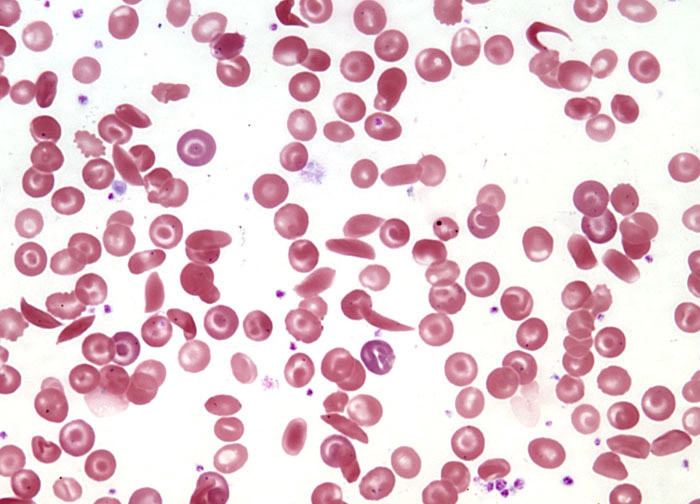
A 6-year-old right-handed boy is brought to the emergency department because of difficulty speaking and inability to raise his right arm. The patient’s mother says his symptoms started suddenly 1 hour ago and have not improved. She says he has never had these symptoms before. No other significant past medical history. The patient was born full-term via spontaneous transvaginal delivery and has met all developmental goals. The family immigrated from Nigeria 3 months ago, and the patient is currently following a vaccination catch-up schedule. His vital signs include: temperature 36.8°C (98.2°F), blood pressure 111/65 mm Hg, pulse 105/min. Height is at the 30th percentile and weight is at the 25th percentile for age and sex. Physical examination is remarkable for generalized pallor, pale conjunctiva, jaundice, and complete loss of strength in the right arm (0/5). His peripheral blood smear is shown in the picture. Which of the following is the most effective preventive measure for this patient’s condition?
A 14-year-old girl is brought to the physician because of a 1-week history of fever, malaise, and chest pain. She describes the pain as 6 out of 10 in intensity and that it is more severe if she takes a deep breath. The pain is centrally located in the chest and does not radiate. Three weeks ago, she had a sore throat that resolved without treatment. She has no personal history of serious illness. She appears ill. Her temperature is 38.7°C (101.7°F). Examination shows several subcutaneous nodules on the elbows and wrist bilaterally. Breath sounds are normal. A soft early systolic murmur is heard best at the apex in the left lateral position. Abdominal examination is unremarkable. Laboratory studies show: Hemoglobin 12.6 g/dL Leukocyte count 12,300/mm3 Platelet count 230,000/mm3 Erythrocyte sedimentation rate 40 mm/hr Serum Antistreptolysin O titer 327 U/mL (N < 200 U/mL) She is treated with aspirin and penicillin and her symptoms resolve. An echocardiography of the heart done 14 days later shows no abnormalities. Which of the following is the most appropriate next step in management?
A 3-year-old boy is brought to the family physician by his parents. They are concerned that he has had multiple nosebleeds in the last 6 months and is always sick compared to other children. During this time period they have also noticed the formation of multiple bruises on his extremities and dry-itching skin on his hands, feet and elbow. On physical exam the physician notes moderate splenomegaly. What is the most likely diagnosis in this child?
A 5-year-old boy is brought to the physician by his parents because of a 4-day history of arthralgias, abdominal pain, and lesions on his arms and legs. Ten days ago, he had an upper respiratory tract infection. A photograph of one of his legs is shown. Further evaluation is most likely to show which of the following?

A 4-year-old boy presents with a history of recurrent bacterial infections, including several episodes of pneumococcal sepsis. His 2 maternal uncles died after having had similar complaints. Lab investigations reveal an undetectable level of all serum immunoglobulins. Which of the following is the most likely diagnosis of this patient?
A 3-year-old boy is brought to the physician for presurgical evaluation before undergoing splenectomy. One year ago, he was diagnosed with hereditary spherocytosis and has received 6 blood transfusions for severe anemia since then. His only medication is a folate supplement. Immunizations are up-to-date. His temperature is 36.7°C (98°F), pulse is 115/min, respirations are 24/min, and blood pressure is 110/60 mm Hg. Examination shows conjunctival pallor and jaundice. The spleen tip is palpated 5 cm below the left costal margin. Which of the following is the most appropriate recommendation to prevent future morbidity and mortality in this patient?
A previously healthy 4-year-old boy is brought to the physician because of blisters and redness on his neck and chest for 2 days. He has also had a fever. He is lethargic and has not eaten well since the rash appeared. He has not had coughing, wheezing, or dysuria. He is an only child and there is no family history of serious illness. His immunizations are up-to-date. His temperature is 38.9°C (102°F), pulse is 90/min, and blood pressure is 80/40 mm Hg. Examination shows flaccid blisters over his neck and trunk that rupture easily. Areas of erythematous moist skin are also noted. Twirling an eraser over the trunk results in a blister. Oropharyngeal examination is normal. Laboratory studies show: Hemoglobin 12 g/dL Leukocyte count 22,000/mm3 Segmented neutrophils 77% Eosinophils 3% Lymphocytes 18% Monocytes 2% Erythrocyte sedimentation rate 60 mm/h Urinalysis is normal. Which of the following is the most likely diagnosis?
A previously healthy 1-year-old boy is brought to the emergency department because of irritability and fever for 2 days. His symptoms began shortly after returning from a family trip to Canada. He was born at term. His immunizations are up-to-date. His 6-year-old brother is healthy and there is no family history of serious illness. The boy appears weak and lethargic. He is at the 50th percentile for height and 75th percentile for weight. His temperature is 39.2°C (102.5°F), pulse is 110/min, respirations are 28/min, and blood pressure is 92/55 mm Hg. Physical examination shows several purple spots over the trunk and extremities that are 1 mm in diameter. Capillary refill time is 4 seconds. The remainder of the examination shows no abnormalities. His hemoglobin concentration is 12 g/dL, leukocyte count is 19,000/mm3, and platelet count is 225,000/mm3. A lumbar puncture is done; cerebrospinal fluid (CSF) analysis shows abundant segmented neutrophils, decreased glucose concentration, and an increased protein concentration. Which of the following is the most appropriate next step in management?
A 10-year-old girl with a rash is brought to the clinic by her mother. The patient’s mother says that the onset of the rash occurred 2 days ago. The rash was itchy, red, and initially localized to the cheeks with circumoral pallor, and it gradually spread to the arms and trunk. The patient’s mother also says her daughter had been reporting a high fever of 39.4°C (102.9°F), headaches, myalgia, and flu-like symptoms about a week ago, which resolved in 2 days with acetaminophen. The patient has no significant past medical history. Her vital signs include: temperature 37.0°C (98.6°F), pulse 90/min, blood pressure 125/85 mm Hg, respiratory rate 20/min. Physical examination shows a symmetric erythematous maculopapular rash on both cheeks with circumoral pallor, which extends to the patient’s trunk, arms, and buttocks. The remainder of the exam is unremarkable. Laboratory findings are significant for a leukocyte count of 7,100/mm3 and platelet count of 325,000/mm3. Which of the following is the next best step in the management of this patient?
Practice by Chapter
Common childhood exanthems
Practice Questions
Pediatric respiratory infections
Practice Questions
Pediatric gastrointestinal infections
Practice Questions
Urinary tract infections in children
Practice Questions
Bone and joint infections
Practice Questions
Central nervous system infections
Practice Questions
Pediatric tuberculosis
Practice Questions
Pediatric HIV
Practice Questions
Recurrent infections evaluation
Practice Questions
Fever of unknown origin approach
Practice Questions
Emerging infectious diseases in children
Practice Questions
Post-infectious immune complications
Practice Questions
Antimicrobial resistance in pediatrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app