
Infectious Disease — MCQs

On this page
A 12-year-old boy presents with recurrent joint pain that migrates from joint to joint and intermittent fever for the last several weeks. He also says that he has no appetite and has been losing weight. The patient is afebrile, and vital signs are within normal limits. On physical examination, he is pale with diffuse petechial bleeding and bruises on his legs. An abdominal examination is significant for hepatosplenomegaly. Ultrasound of the abdomen confirms hepatosplenomegaly and also shows multiple enlarged mesenteric lymph nodes. A complete blood count (CBC) shows severe anemia and thrombocytopenia with leukocytosis. Which of the following is the most likely diagnosis in this patient?
A 12-year-old boy is brought in by his mother to the emergency department. He has had abdominal pain, fever, nausea, vomiting, and loss of appetite since yesterday. At first, the mother believed it was just a "stomach flu," but she is growing concerned about his progressive decline. Vitals include: T 102.3 F, HR 110 bpm, BP 120/89 mmHg, RR 16, O2 Sat 100%. Abdominal exam is notable for pain over the right lower quadrant. What is the next best step in management in addition to IV hydration and analgesia?
A 7-year-old boy with a past medical history significant only for prior head lice infection presents to the clinic after being sent by the school nurse for a repeat lice infection. The boy endorses an itchy scalp, but a review of systems is otherwise negative. After confirming the child’s diagnosis and sending him home with appropriate treatment, the school nurse contacts the clinic asking for recommendations on how to prevent future infection. Which of the following would be the best option to decrease the likelihood of lice reinfestation?
A previously healthy 5-year-old boy is brought to the physician by his parents because of a 2-day history of poor balance and difficulty walking. He has fallen multiple times and is unable to walk up the stairs unassisted. He has also had difficulty tying his shoes and dressing himself. His family adheres to a vegetarian diet. He has not yet received any routine childhood vaccinations. His mother has a history of anxiety. He is at the 70th percentile for height and 30th percentile for weight. Vital signs are within normal limits. He is alert and oriented to person, place, and time. Physical examination shows a broad-based, staggering gait. He has difficulty touching his nose and cannot perform rapidly-alternating palm movements. Strength is 5/5 in the upper and lower extremities. Deep tendon reflexes are 1+ bilaterally. Skin examination shows several faint hyperpigmented macules on the chest. Which of the following is the most likely underlying cause of this patient's symptoms?
A 5-year-old girl is brought to the physician by her mother because of a 3-week history of a foul-smelling discharge from the left nostril. There was one episode of blood-tinged fluid draining from the nostril during this period. She has been mouth-breathing in her sleep for the past 4 days. She was born at term. Her 1-year-old brother was treated for viral gastroenteritis 3 weeks ago. She is at 60th percentile for height and at 70th percentile for weight. Her temperature is 37°C (98.6°F), pulse is 96/min, respirations are 23/min, and blood pressure is 96/54 mm Hg. Examination shows mucopurulent discharge in the left nasal cavity. Oral and otoscopic examination is unremarkable. Endoscopic examination of the nose confirms the diagnosis. Which of the following is the most appropriate next step in management?
A 4-year-old girl is brought to the physician because of a nonpruritic, painless rash that has been on her face for 5 days. She was born at term and has been healthy throughout childhood. Her 62-year-old maternal grandmother has bullous pemphigoid. Her development is adequate for her age and immunizations are up-to-date. She appears healthy and well-nourished. Her temperature is 37.0°C (98.6°F) pulse is 90/min, and respiratory rate is 18/min. Examination shows a crusted rash on the right side of the patient's face. An image of the patient's lower face is shown. The remainder of the examination shows no abnormalities. Which of the following is the most appropriate next step in management?

A 3-year-old boy is brought to the emergency department because of persistent fever and cough. Three days ago, he was diagnosed with pneumonia and acute otitis media. He was started on ampicillin-sulbactam and clarithromycin, but his symptoms did not improve. The mother reports that her son has been hospitalized 3 times due to pneumonia. He was first diagnosed with pneumonia at the age of 10 months. She also reports several episodes of bilateral otitis media and recurrent respiratory tract infections. His immunizations are up-to-date. He is at the 50th percentile for height and 20th percentile for weight. He appears fatigued. His temperature is 38°C (100.4°F). Pneumatic otoscopy shows purulent otorrhea bilaterally. Pulmonary examination shows decreased breath sounds over both lung fields. The palatine tonsils and adenoids are hypoplastic. Which of the following is the most likely underlying cause of this patient's condition?
A 16-year-old boy comes to the emergency department because of painful urination and urethral discharge for 3 days. He has multiple sexual partners and only occasionally uses condoms. His vital signs are within normal limits. The result of nucleic acid amplification testing for Neisseria gonorrhoeae is positive. The patient requests that his parents not be informed of the diagnosis. Which of the following initial actions by the physician is most appropriate?
An 8-month-old girl is brought to the emergency department because of fever, vomiting, and diarrhea for 3 days. Her parents report at least 10 watery stools daily. She has had three upper respiratory tract infections since she started daycare 2 months ago, but has otherwise been developing normally. Her mother has a history of celiac disease. The patient is at the 57th percentile for height and the 65th percentile for weight. Her immunizations are incomplete. Her temperature is 38.5°C (101.3°F), pulse is 145/min, and blood pressure is 92/54 mm Hg. Examination shows dry mucous membranes and decreased skin turgor. Bowel sounds are hyperactive. A complete blood count and serum concentrations of glucose, urea nitrogen, and creatinine are within the reference range; there is hypokalemia. In addition to intravenous fluid resuscitation, which of the following is the most appropriate next step in management?
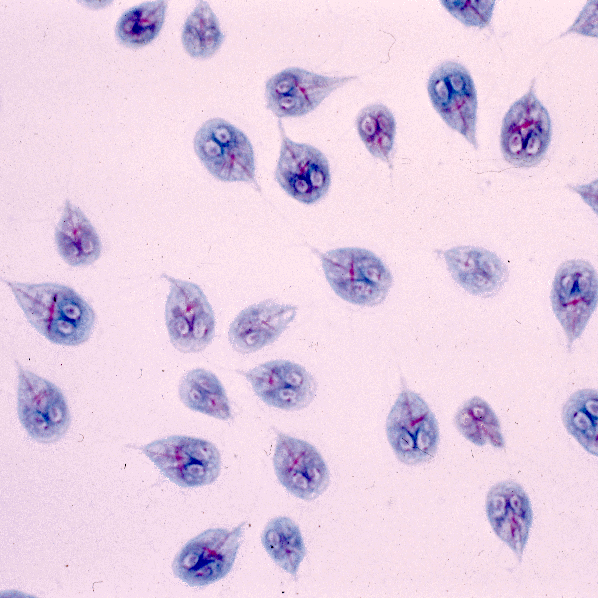
A 5-year-old boy is brought to the physician because of intermittent abdominal cramps and recurrent episodes of foul-smelling greasy diarrhea for 3 months. He has a history of recurrent upper respiratory infection. The abdomen is diffusely tender to palpation and resonant to percussion. Laboratory studies show markedly reduced IgA with normal IgG and IgM levels. A photomicrograph of a stool sample is shown. This patient is at increased risk for which of the following?
Practice by Chapter
Common childhood exanthems
Practice Questions
Pediatric respiratory infections
Practice Questions
Pediatric gastrointestinal infections
Practice Questions
Urinary tract infections in children
Practice Questions
Bone and joint infections
Practice Questions
Central nervous system infections
Practice Questions
Pediatric tuberculosis
Practice Questions
Pediatric HIV
Practice Questions
Recurrent infections evaluation
Practice Questions
Fever of unknown origin approach
Practice Questions
Emerging infectious diseases in children
Practice Questions
Post-infectious immune complications
Practice Questions
Antimicrobial resistance in pediatrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app