
Infectious Disease — MCQs

On this page
A 4-year-old boy is brought to the pediatrician with fever, diarrhea and bilateral red eye for 7 days. His parents noted that he has never had an episode of diarrhea this prolonged, but several other children at daycare had been ill. His immunization history is up to date. His vitals are normal except for a temperature of 37.5°C (99°F). A physical exam is significant for mild dehydration, preauricular adenopathy, and bilateral conjunctival injection with watery discharge. What is the most likely diagnosis?
A 2-year-old girl is brought to her pediatrician’s office with intermittent and severe stomach ache and vomiting for the last 2 days. Last week the whole family had a stomach bug involving a few days of mild fever, lack of appetite, and diarrhea but they have all made a full recovery since. This current pain is different from the type she had during infection. With the onset of pain, the child cries and kicks her legs up in the air or pulls them to her chest. The parents have also observed mucousy stools and occasional bloody stools that are bright red and mucousy. After a while, the pain subsides and she returns to her normal activity. Which of the following would be the next step in the management of this patient?
A mother brings her 6-month-old boy to the emergency department. She reports that her son has been breathing faster than usual for the past 2 days, and she has noted occasional wheezing. She states that prior to the difficulty breathing, she noticed some clear nasal discharge for several days. The infant was born full-term, with no complications, and no significant medical history. His temperature is 100°F (37.8°C), blood pressure is 60/30 mmHg, pulse is 120/min, respirations are 40/min, and oxygen saturation is 95% on room air. Physical exam reveals expiratory wheezing, crackles diffusely, and intercostal retractions. The child is currently playing with toys. Which of the following is the most appropriate next step in management?
An 8-year-old boy with asthma is brought to the physician because of a 2-week history of facial pain and congestion. His mother states that the nasal discharge was initially clear, but it has become thicker and more purulent over the last week. He has tried multiple over-the-counter oral decongestants and antihistamines, with minimal relief. Current medications include cetirizine, intranasal oxymetazoline, and albuterol. His temperature is 37.7°C (99.8°F), pulse is 100/min, respirations are 14/min, and blood pressure is 110/70 mm Hg. Examination shows congested nasal mucosa with purulent discharge from the nares bilaterally. There is tenderness to palpation over the cheeks, with no transillumination over the maxillary sinuses. Which of the following is the most likely predisposing factor for this patient's current condition?
A 9-month-old girl is brought to the emergency department because of a 3-day history of fever, irritability, and discharge from her right ear. She had an episode of ear pain and fever three weeks ago. Her parents did not seek medical advice and the symptoms improved with symptomatic treatment. There is no family history of frequent infections. She appears ill. Her temperature is 39.3°C (102.7°F). Physical examination shows erythema and tenderness in the right postauricular region, and lateral and inferior displacement of the auricle. Otoscopy shows a bulging and cloudy tympanic membrane, with pus oozing out. The remainder of the examination shows no abnormalities. Laboratory studies show: Hemoglobin 11.5 g/dL Leukocyte count 15,800/mm3 Segmented neutrophils 80% Eosinophils 1% Lymphocytes 17% Monocytes 2% Platelet count 258,000/mm3 Which of the following is the most appropriate next step in management?
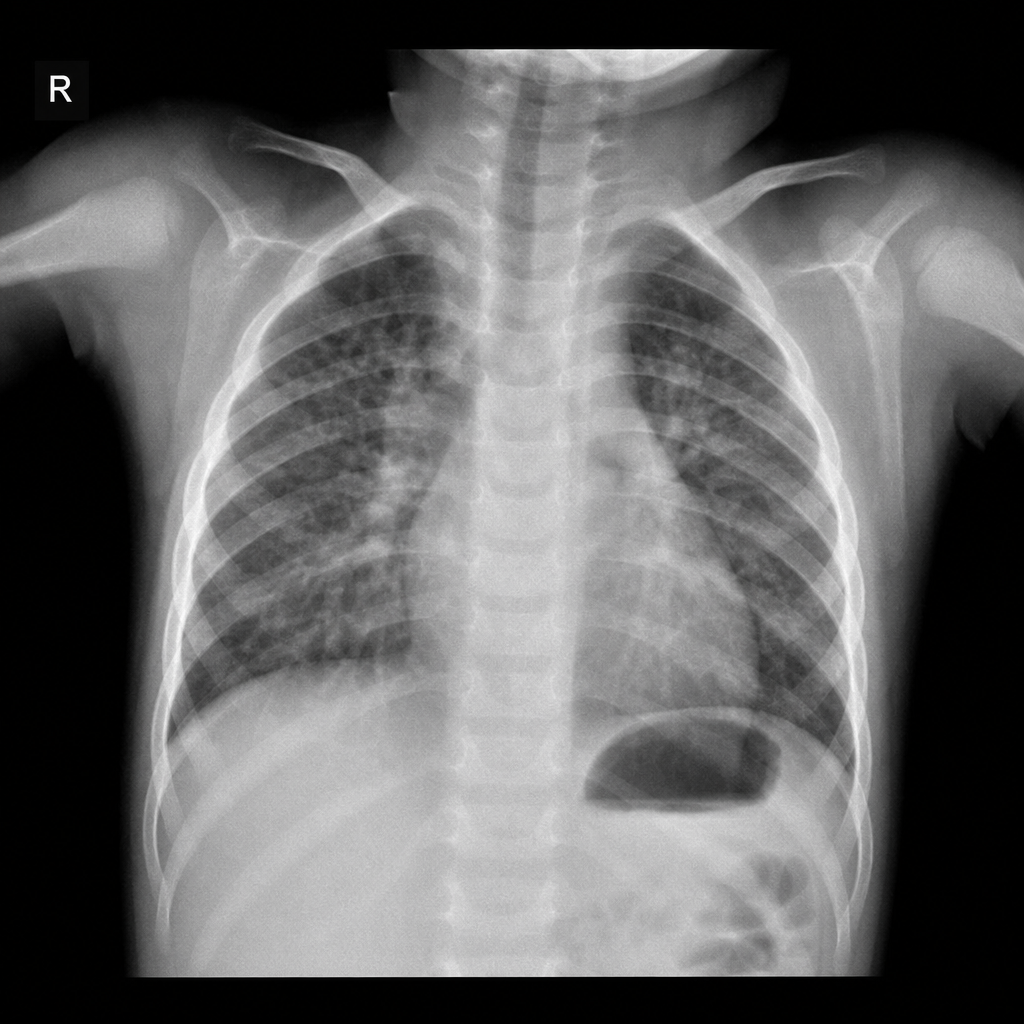
An 18-month-old girl is brought to the emergency room by her mother because of wheezing for 1 day. The baby has never had similar symptoms. She also has a runny nose and a cough. She is not feeding well. Her immunizations are up-to-date. Her rectal temperature is 38.8°C (101.8°F), the heart rate is 120/min, and the respiratory rate is 23/min. On examination, a clear nasal discharge is noticed with intercostal retractions. Chest auscultation reveals bilateral fine rales and diffuse fine wheezing. A chest X-ray is given in the exhibit. What is the most likely diagnosis?
A 3-year-old boy is brought to the emergency department after the sudden onset of a rash that started on the head and progressed to the trunk and extremities. Over the past week, he has had a runny nose, a cough, and red, crusty eyes. He recently immigrated with his family from Yemen and immunization records are unavailable. The patient appears malnourished. His temperature is 40.0°C (104°F). Examination shows generalized lymphadenopathy and a blanching, partially confluent maculopapular exanthema. Administration of which of the following is most likely to improve this patient's condition?
A 9-year-old girl presents with dyspnea, palpitations, joint pain, and fever for the past week. She says that her symptoms started 2 weeks ago with bilateral knee pain which has shifted to both ankles over the past week. She says she noticed bilateral leg swelling since yesterday. Past medical history is significant for a severe sore throat, fever, chills, and myalgia 1 month ago which resolved after a week. Her vital signs include: respiratory rate 22/min, temperature 37.7°C (100.0°F), blood pressure 90/60 mm Hg, pulse 90/min, and SpO2 88% on room air. On physical examination, the patient is ill-appearing with pallor and bilateral pitting edema of legs. The apex beat is prominently located in the 5th intercostal space in the mid-axillary line. Crepitus is noted over both lung bases bilaterally. A loud 3/6 pansystolic murmur is heard at the apex radiating towards the axilla. S3 and S4 sounds are noted at the left sternal border and cardiac apex. Which of the following is the most likely diagnosis in this patient?
A 5-year-old boy is brought to the emergency department by his mother because of a 2-hour history of word-finding difficulty, speech slurring, and weakness and sensory loss of his right arm and leg. He has not had fever, nausea, headache, or diarrhea. His mother reports an episode of severe pain and soft tissue swelling of the dorsum of his hands and feet when he was 12 months old, which self-resolved after 2 weeks. His temperature is 37.7°C (99.8°F), pulse is 90/min, and blood pressure is 110/80 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 91%. He follows commands but has nonfluent aphasia. Examination shows marked weakness and decreased sensation of the right upper and lower extremities. Deep tendon reflexes are 2+ bilaterally. Babinski sign is present on the right. An MRI scan of the brain shows signs of an evolving cerebral infarction on the patient's left side. Which of the following is the most appropriate initial step in management?
A 3-year-old girl presents to the emergency department with skin desquamation over her hips and buttocks and right arm; she also has conjunctivitis and fever. The patient was previously seen by her pediatrician for symptoms of impetigo around the nasal folds, and she was treated with topical fusidic acid. She was born at 39 weeks’ gestation via spontaneous vaginal delivery, is up to date on all vaccines, and is meeting all developmental milestones. Medical history and family history are unremarkable. She is admitted to the hospital and started on IV antibiotics. Today, her blood pressure is 100/60 mm Hg, heart rate is 100 beats per minute, respiratory rate is 22 breaths per minute, and temperature is 39.4°C (102.9°F). The total area of desquamation exceeds 20%, sparing the mucous membranes. She is transferred to the pediatric intensive care unit. What is the most likely cause of the disease?
Practice by Chapter
Common childhood exanthems
Practice Questions
Pediatric respiratory infections
Practice Questions
Pediatric gastrointestinal infections
Practice Questions
Urinary tract infections in children
Practice Questions
Bone and joint infections
Practice Questions
Central nervous system infections
Practice Questions
Pediatric tuberculosis
Practice Questions
Pediatric HIV
Practice Questions
Recurrent infections evaluation
Practice Questions
Fever of unknown origin approach
Practice Questions
Emerging infectious diseases in children
Practice Questions
Post-infectious immune complications
Practice Questions
Antimicrobial resistance in pediatrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app