
Infectious Disease — MCQs

On this page
A 3-day-old term male neonate developed progressive respiratory distress and cyanosis unresponsive to supplemental oxygen delivered by nasal cannula. On examination, the cardiac point of maximal impulse is located at the right sternal border, and breath sounds are diminished over the left hemithorax. The abdomen appears scaphoid. Which of the following is the most appropriate immediate next step in management?

A 4-year-old boy presents with low-grade fever, inspiratory stridor, and barking cough for the past 5 days. Examination reveals a hoarse voice, a moderately inflamed pharynx, and a slightly increased respiratory rate. His chest x-ray showed subglottic narrowing appearing like a steeple. Which among the following is not indicated in the treatment of this condition?
A child presents with recurrent infections. Mediastinal imaging reveals an absent thymus gland, and further investigations show low ADA (adenosine deaminase) levels. What is the most likely diagnosis?
A 6-year-old child presents to the emergency department with sudden onset of palpitations, shortness of breath, and dizziness. The child has no significant past medical history. On examination, the heart rate is 220 beats per minute, blood pressure is $90 / 60 \mathrm{mmHg}$, and the child appears anxious but is otherwise stable. An ECG confirms the diagnosis of paroxysmal supraventricular tachycardia (PSVT). What is the initial recommended dose of adenosine for this child?
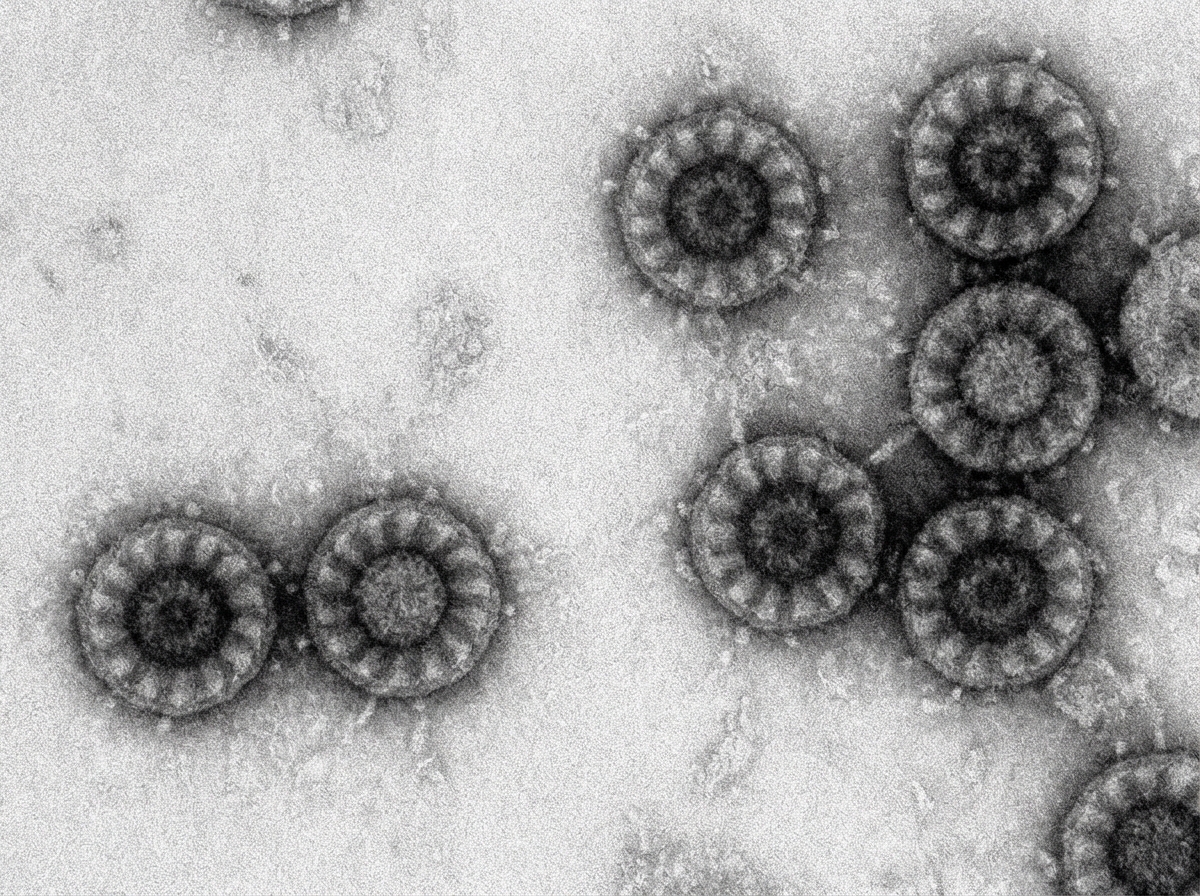
A 2 year old child came with watery diarrhea. Electron Microscopy (EM) Image is shown here. Choose the correct pathogen.
An unimmunized 5 -year-old child presents to the OPD with a white membranous layer on the throat upon inspection. The child's brother is immunized. What is the first step in management?
A 2-year-old male is brought to your office by his mother for evaluation. The patient develops a skin presentation similar to Image A on his cheeks and chin when exposed to certain food products. This patient is most likely predisposed to develop which of the following?

A 4-year-old boy who otherwise has no significant past medical history presents to the pediatric clinic accompanied by his father for a 2-day history of high fever, sore throat, nausea, vomiting, and bloody diarrhea. The patient’s father endorses that these symptoms began approximately 3 weeks after the family got a new dog. His father also states that several other children at the patient’s preschool have been sick with similar symptoms. He denies any other recent changes to his diet or lifestyle. The patient's blood pressure is 123/81 mm Hg, pulse is 91/min, respiratory rate is 15/min, and temperature is 39.2°C (102.5°F). Which of the following is the most likely cause for this patient’s presentation?
A 4-year-old girl presents to a pediatrician for a scheduled follow-up visit. She was diagnosed with her first episode of acute otitis media 10 days ago and had been prescribed oral amoxicillin. Her clinical features at the time of the initial presentation included pain in the ear, fever, and nasal congestion. The tympanic membrane in the left ear was markedly red in color. Today, after completing 10 days of antibiotic therapy, her parents report that she is asymptomatic, except for mild fullness in the left ear. There is no history of chronic nasal obstruction or chronic/recurrent rhinosinusitis. On physical examination, the girl's vital signs are stable. Otoscopic examination of the left ear shows the presence of an air-fluid interface behind the translucent tympanic membrane and decreased mobility of the tympanic membrane. Which of the following is the next best step in the management of this patient?
A 3-year-old girl is brought to the emergency room because of a 5-day history of high fever and fatigue. During this time she has been crying more than usual and eating less. Her mother says that the child has also complained about pain in her arms and legs for the past 3 days. She was born at term and has been otherwise healthy. She appears ill. Her temperature is 39.5°C (103.1°F), pulse is 128/min, and blood pressure is 96/52 mm Hg. The lungs are clear to auscultation. A grade 3/6 systolic murmur is heard at the apex. There is mild tenderness to palpation of the left upper quadrant with no guarding or rebound. The spleen is palpated 3 cm below the left costal margin. There is no redness or swelling of the joints. Laboratory studies show: Hemoglobin 11.8 g/dL Leukocyte count 16,300/mm3 Platelet count 220,000/mm3 Erythrocyte sedimentation rate 50 mm/h Serum Glucose 96 mg/dL Creatinine 1.7 mg/dL Total bilirubin 0.4 mg/dL AST 18 U/L ALT 20 U/L Urine Protein 2+ RBC casts rare RBC 10/hpf WBC 1–2/hpf Which of the following is the most appropriate next step in management?
Practice by Chapter
Common childhood exanthems
Practice Questions
Pediatric respiratory infections
Practice Questions
Pediatric gastrointestinal infections
Practice Questions
Urinary tract infections in children
Practice Questions
Bone and joint infections
Practice Questions
Central nervous system infections
Practice Questions
Pediatric tuberculosis
Practice Questions
Pediatric HIV
Practice Questions
Recurrent infections evaluation
Practice Questions
Fever of unknown origin approach
Practice Questions
Emerging infectious diseases in children
Practice Questions
Post-infectious immune complications
Practice Questions
Antimicrobial resistance in pediatrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app