
Congenital defects — MCQs

On this page
A 2720-g (6-lb) female newborn is delivered at term to a 39-year-old woman, gravida 3, para 2. Examination in the delivery room shows micrognathia, prominent occiput with flattened nasal bridge, and pointy low-set ears. The eyes are upward slanting with small palpebral fissures. The fists are clenched with fingers tightly flexed. The index finger overlaps the third finger and the fifth finger overlaps the fourth. A 3/6 holosystolic murmur is heard at the lower left sternal border. The nipples are widely spaced and the feet have prominent heels and convex, rounded soles. Which of the following is the most likely cause of these findings?
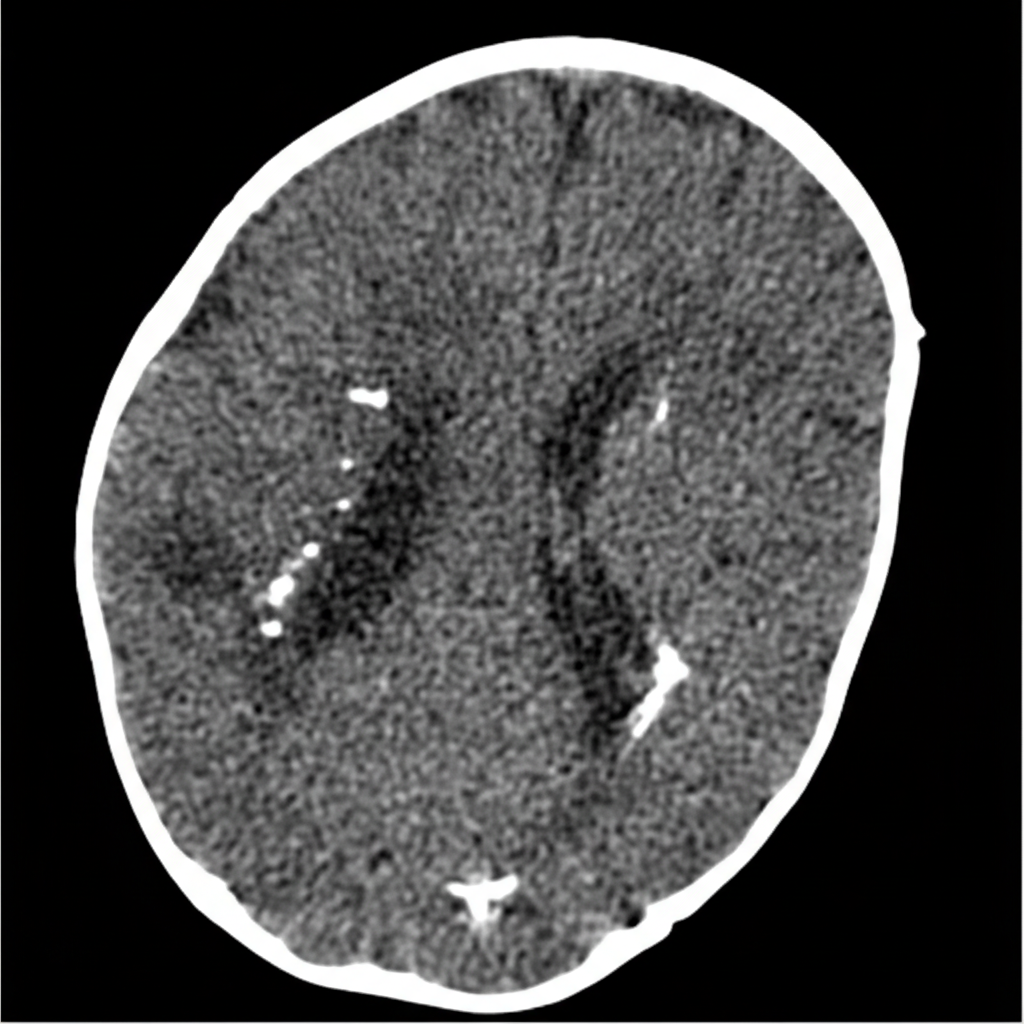
A 2-day-old boy, born at 38-weeks gestation, presents with jaundice and microcephaly. Social history reveals his mother is an animal caretaker. The vital signs include: temperature 37.0°C (98.6°F), blood pressure 75/40 mm Hg, pulse 150/min, respiratory rate 40/min, and oxygen saturation 99% on room air. Physical examination reveals hepatosplenomegaly. A CT and MRI of the head are significant for the following findings (see picture). Which of the following diseases contracted during pregnancy is the most likely cause of this patient's condition?
A 3000-g (6-lb 10-oz) male newborn delivered at 38 weeks' gestation develops respiratory distress shortly after birth. Physical examination shows low-set ears, retrognathia, and club feet. Within a few hours, the newborn dies. Examination of the liver at autopsy shows periportal fibrosis. Which of the following is the most likely underlying cause of the neonate's presentation?
A 2-month-old infant boy is brought into the clinic for a well-child check. Mom reports a healthy pregnancy with no complications. Though she said the ultrasound technician saw “some white deposits in his brain” during a prenatal check, mom was not concerned. The baby was delivered at 38 weeks of gestation during a home birth. When asked if there were any problems with the birthing process, mom denied any difficulties except that “he was small and had these blue dots all over.” Physical exam was unremarkable except for the absence of object tracking. What other finding would you expect?
A 4-year-old girl is being followed by the pediatric oncology team after her pediatrician found a palpable abdominal mass towards the right flank 2 weeks ago. Abdominal ultrasonography detected a solid mass in the right kidney without infiltration of the renal vein and inferior vena cava. The contrast-enhanced computed tomography (CT) confirmed the presence of a solitary mass in the right kidney surrounded by a pseudocapsule consisting of a rim of normal tissue, displacing it medially, and distorting the collecting system. No nodal involvement was detected. In which of the following chromosomes would you expect a genetic abnormality?
A 3175-g (7-lb) female newborn is delivered at term. Initial examination shows a distended abdomen and a flat perineal region without an opening. A dark green discharge is coming out of the vulva. Which of the following is the most likely diagnosis?
A 7-year-old Caucasian girl with asthma presents to her pediatrician with recurrent sinusitis. The patient’s mother states that her asthma seems to be getting worse and notes that ‘lung problems run in the family’. The patient has had 2 episodes of pneumonia in the last year and continues to frequently have a cough. Her mother says that 1 of her nieces was recently diagnosed with cystic fibrosis. On physical examination, the child has clubbing of the nail beds on both hands. A chloride sweat test is performed on the patient, and the child’s sweat chloride concentration is found to be within normal limits. The physician is still suspicious for cystic fibrosis and believes the prior asthma diagnosis is incorrect. Which of the following diagnostic tests would aid in confirming this physician’s suspicions?
A 7-year-old boy is being evaluated in pediatric cardiology clinic. He appears grossly normal, but suddenly becomes tachypneic and cyanotic when his mom takes a toy away from him. These symptoms resolve somewhat when he drops into a squatting position. Transthoracic echocardiography reveals pulmonic stenosis, a ventricular septal defect, right ventricular hypertrophy, and an overriding aorta. Which of the following best predicts the degree of cyanosis and other hypoxemic symptoms in this patient?
A 3400-g (7-lb 8-oz) female newborn is delivered at term to a 28-year-old primigravid woman. Apgar scores are 7 and 8 at 1 and 5 minutes, respectively. Vital signs are within normal limits. Examination shows swelling of bilateral upper and lower extremities and low-set ears. The posterior hair line is low and the chest appears broad. There are skin folds running down the sides of the neck to the shoulders. A grade 2/6 systolic ejection murmur and systolic click is heard at the apex. Which of the following is the most likely cause of this patient's swelling?
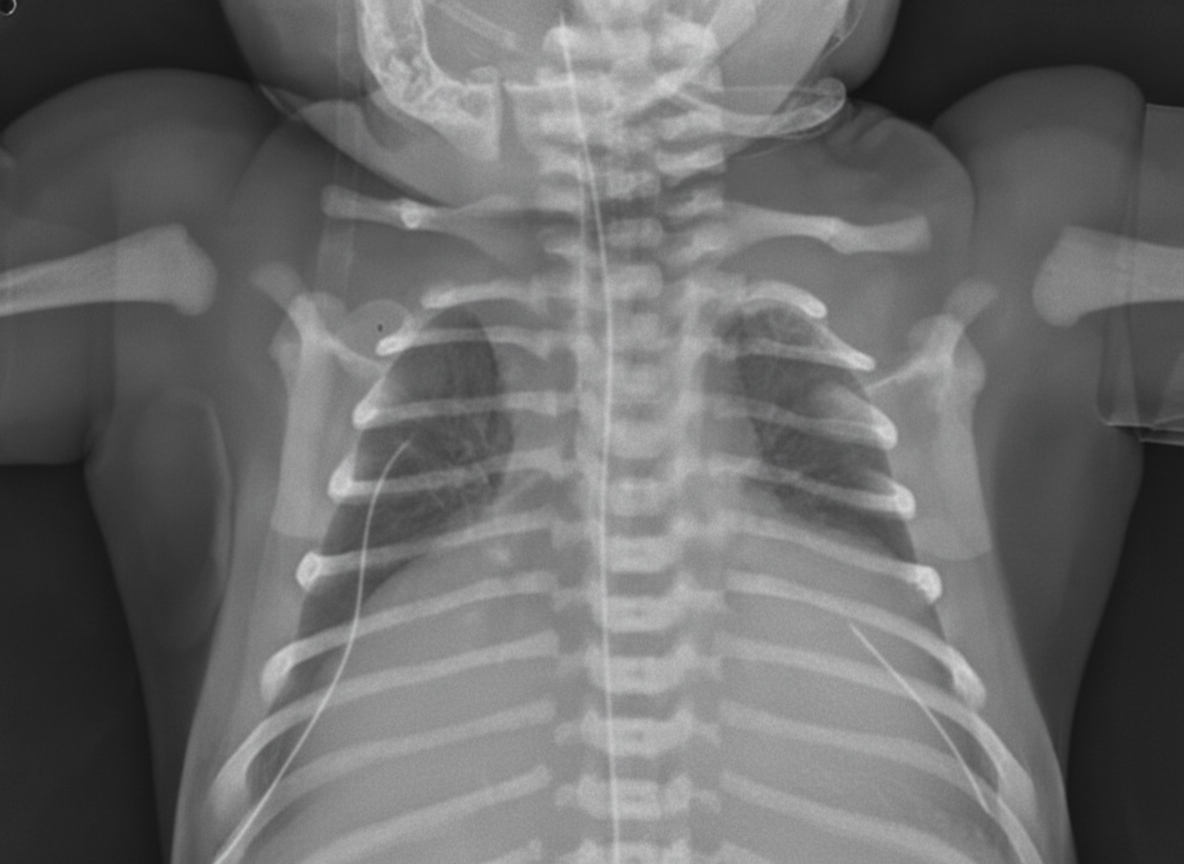
A 2-hours-old neonate is found to have bluish discoloration throughout his body, including lips and tongue. The boy was born at 39 weeks gestation via spontaneous vaginal delivery with no prenatal care. Maternal history is positive for type 2 diabetes mellitus for 11 years. On physical examination, his blood pressure is 55/33 mm Hg, his heart rate is 150/min, respiratory rate is 45/min, temperature of 37°C (98.6°F), and oxygen saturation is 84% on room air. Appropriate measures are taken. Auscultation of the chest reveals a single second heart sound without murmurs. Chest X-ray is shown in the exhibit. Which of the following is the most likely diagnosis?
Practice by Chapter
Neural tube defects
Practice Questions
Congenital heart defects
Practice Questions
Gastrointestinal malformations
Practice Questions
Genitourinary anomalies
Practice Questions
Craniofacial anomalies
Practice Questions
Skeletal dysplasias
Practice Questions
Chromosomal disorders
Practice Questions
Teratogenic exposures
Practice Questions
Multiple malformation syndromes
Practice Questions
Prenatal diagnosis of congenital defects
Practice Questions
Surgical management timing
Practice Questions
Long-term outcomes and follow-up
Practice Questions
Preventive strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app