
Congenital defects — MCQs

On this page
A 4-week-old newborn is brought to the physician for a well-child examination. He was born at 40 weeks' gestation and weighed 3300 g (7 lb 4 oz). He now weighs 4300 g (9 lbs 1 oz). There is no family history of serious illness. He is at the 50th percentile for height and 50th percentile for weight. Vital signs are within normal limits. Examination shows a grade 3/6 harsh holosystolic murmur at the left lower sternal border and a soft mid-diastolic murmur over the cardiac apex. The lungs are clear to auscultation. The remainder of the examination shows no abnormalities. Which of the following is the most likely explanation for this patient's physical findings?
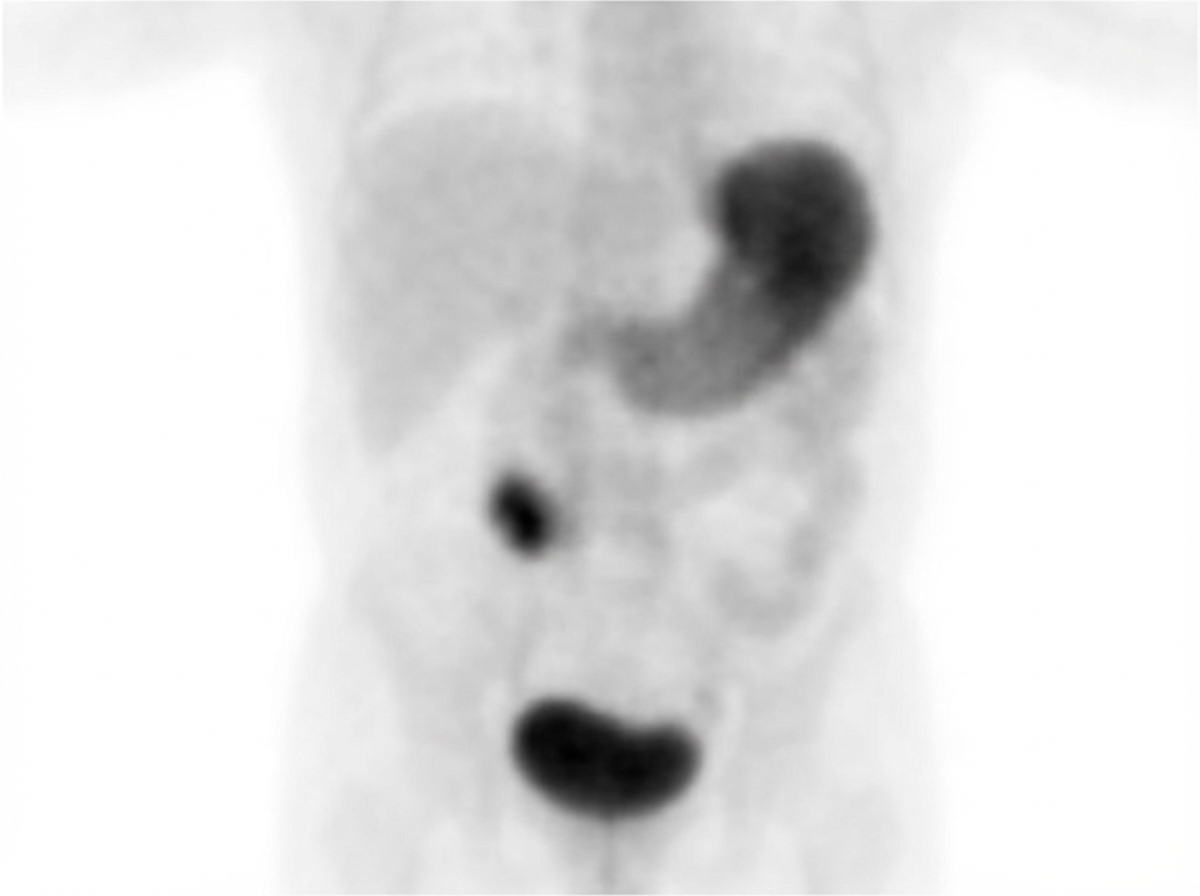
A 2-year-old, previously healthy female presents to the emergency department complaining of 7 hours of 10/10 intermittent abdominal pain, vomiting, and dark red stools. On exam, there is tenderness to palpation in the right lower quadrant and high-pitched bowel sounds. Technetium-99m pertechnetate scan was performed (Image A). Which of the following is true about this patient's condition?
A 2-year-old boy is brought to the emergency department because of a 5-minute episode of repetitive, involuntary, twitching movements of his left arm that occurred 1 hour ago. His symptoms began while playing with some toys. His parents say that he began to stand with support at 18 months and has recently started to walk with support. He speaks in bisyllables. He is at the 70th percentile for length and 80th percentile for weight. His vital signs are within normal limits. Examination shows a purple-pink patch over the right cheek that extends to the right eyelid. The right eyeball is firm. Neurologic examination shows left arm hypotonia and absent bicep reflex on the left side. Fundoscopy shows cupping of the right optic disc. Which of the following is the most likely cause of this patient's symptoms?
A 4-month-old infant girl is brought to the pediatrician because of feeding problems and recurrent infections. She has a blood pressure of 104/65 mm Hg and heart rate of 91/min. On physical examination, she has a cleft palate, malformed jaw, structural cardiac abnormalities, and diminished cell-mediated responses. Laboratory investigations reveal hypocalcemia. Which of the following is the most likely diagnosis?
A 14-year-old girl presents to the pediatrician because she has not experienced the onset of menstruation. Her mother reports that her pubic hair developed at the age of 9 years. Her mother also informs that she has been experiencing recurrent serous otitis media since early childhood. The temperature is 36.8°C (98.4°F), pulse is 88/min, blood pressure is 128/78 mm Hg, and respiratory rate is 14/min. The physical examination shows hypoplastic nails, along with short 4th and 5th metacarpals, and cubitus valgus bilaterally. In addition, the examination of her chest shows lack of breast development with widely spaced nipples. The auscultation of the chest reveals normal heart sounds with no murmur noted. The examination of the head and neck region shows a high arched palate, dental malocclusion, and a low hairline. Which of the following signs is most likely to be present on examination of her skin?
A 16-year-old teenager is brought to the pediatrician's office by her mother. The mother expresses concerns about her daughter's health because she has not achieved menarche. The daughter confirms this and upon further questioning, denies any significant weight loss, changes in mood, or changes in her appetite. She denies being sexually active. She is a good student who works hard and enjoys competing in sports. She was born via spontaneous vaginal delivery at 39 weeks. There was some discussion about mild birth defects, but her mother never followed up and can not recall the specifics. Her vaccines are up to date and she has met all developmental milestones. Past medical history and family history are benign. She has a heart rate of 90/min, respiratory rate of 17/min, blood pressure of 110/65 mm Hg, and temperature of 37.0°C (98.6°F). On physical examination, the patient is short in stature at the 33rd percentile in height. Additionally, she has some excessive skin in the neck and has a broad chest with widely spaced nipples. A urine pregnancy test is negative. Which of the following genetic abnormalities is the most likely cause of this patient's condition?
A healthy 37-year-old gravida-3-para-1 (G-3-P-1) who underwent in vitro fertilization delivers a boy vaginally. On examination, he is found to have a ventral urethral meatus inferior to the glans. Which statement is correct?
A 7-year-old girl is brought to the physician with complaints of recurrent episodes of dysuria for the past few months. Her parents reported 4 to 5 similar episodes in the last year. They also note that she has had several urinary tract infections throughout her childhood. She has no other medical problems and takes no medications. Her temperature is 38.6ºC (101.4°F), pulse is 88/min, and respiratory rate is 20/min. On physical examination, suprapubic tenderness is noted. On ultrasonography, hydronephrosis and scarring are present. Which of the following is the most appropriate next step?
A 2-year-old boy is brought to the physician by his father for a well-child examination. He recently emigrated from Mexico with his family and has not seen a physician since birth. Vital signs are within normal limits. Cardiac examination shows a harsh, grade 3/6 holosystolic murmur heard best at the left lower sternal border. During deep inspiration, the second heart sound is split. If left untreated, irreversible changes would most likely be seen in which of the following structures?
A 6-month-old infant girl is brought by her parents to the emergency room due to abnormal jerky movements of the upper and lower limbs for the past month. When questioned about her birth history, the parents mention that a prenatal scan of the fetal heart revealed that the patient had a mass in the left ventricle, which led to the diagnosis of a neurocutaneous disorder in the child. Which of the following findings is a characteristic cutaneous finding associated with this young patient’s disorder?
Practice by Chapter
Neural tube defects
Practice Questions
Congenital heart defects
Practice Questions
Gastrointestinal malformations
Practice Questions
Genitourinary anomalies
Practice Questions
Craniofacial anomalies
Practice Questions
Skeletal dysplasias
Practice Questions
Chromosomal disorders
Practice Questions
Teratogenic exposures
Practice Questions
Multiple malformation syndromes
Practice Questions
Prenatal diagnosis of congenital defects
Practice Questions
Surgical management timing
Practice Questions
Long-term outcomes and follow-up
Practice Questions
Preventive strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app