
Congenital defects — MCQs

On this page
A 6-week-old girl is brought to the physician for a follow-up examination. She has had difficulty feeding with frequent regurgitation of milk and her mother is concerned that the child is not gaining weight appropriately. The mother reports that the girl's crying resembles a squeaky door. She is at the 2nd percentile for head circumference, 30th percentile for height, and 15th percentile for weight. Examination shows mandibular hypoplasia, a broad nasal bridge, widely-spaced eyes, and a round face. The palpebral fissures are down-slanting and she has a single palmar crease. A 3/6 pansystolic murmur is heard along the left lower sternal border. Which of the following is the most likely cause of this patient's symptoms?
An otherwise healthy 8-year-old girl is brought to the physician by her parents because of concern for growth retardation. Although she has always been short for her age, her classmates have begun teasing her for her height. She is at the 5th percentile for height and 25th percentile for weight. Physical examination shows a low-set posterior hairline, increased skin folds along the side of the neck, and a high-arched palate. The nipples are widely spaced and the fourth metacarpal bones are shortened bilaterally. This patient is at increased risk of developing which of the following complications?
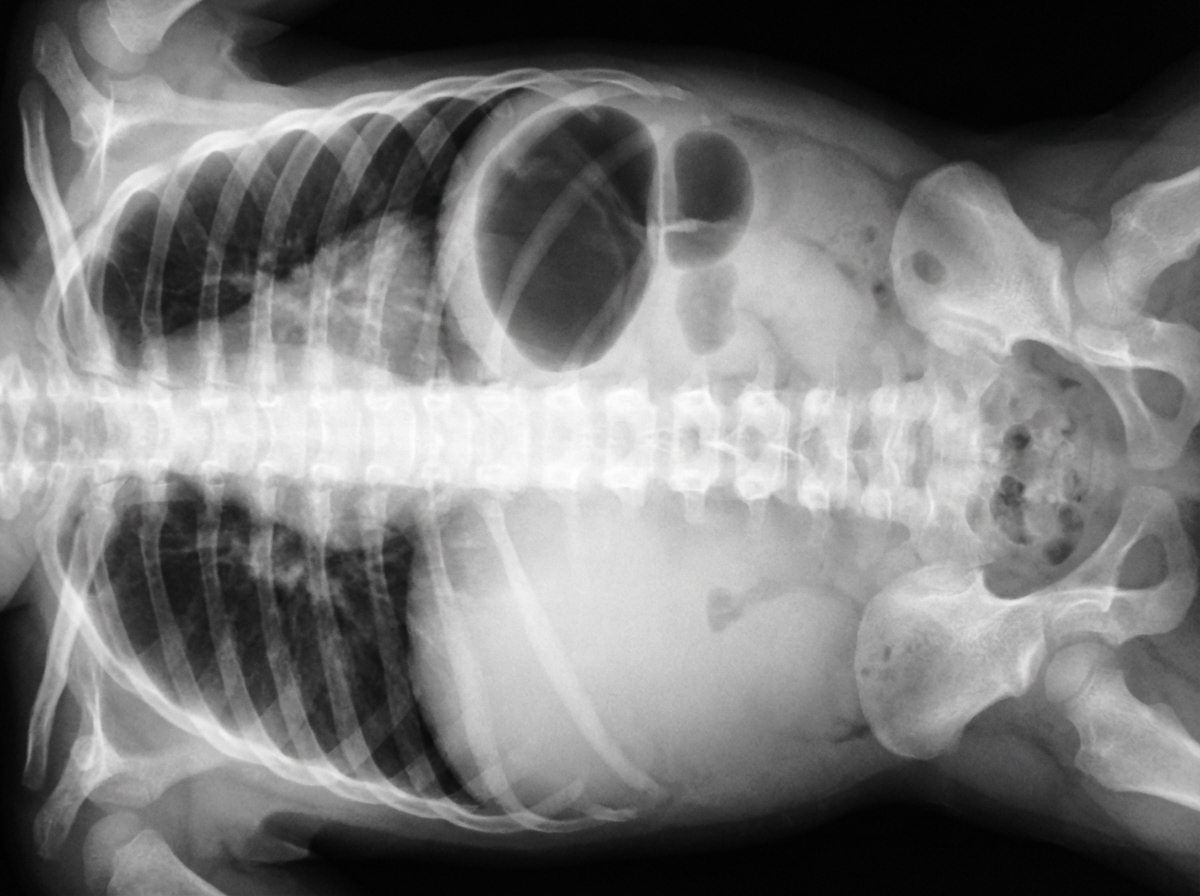
A female newborn delivered at 38 weeks’ gestation is evaluated for abdominal distention and bilious vomiting 24 hours after delivery. The pregnancy and delivery were uncomplicated. She appears lethargic and her fontanelles are sunken. An x-ray of the abdomen is shown. This infant most likely has a congenital obstruction affecting which of the following anatomic structures?
A 16-year-old boy is brought to the physician by his parents because of a 6-month history of progressive fatigue and worsening shortness of breath on exertion. The parents report that the boy “has always been tired out a bit more easily than other kids.” The family recently immigrated to the United States from rural South Korea. Pulse oximetry on room air shows an oxygen saturation of 96% on bilateral index fingers. Radial pulses are bounding. There is mild bluish discoloration and bulbous enlargement of the distal toes bilaterally. Echocardiography is most likely to show which of the following?
A 2-year-old boy is brought to the physician because of progressive difficulty breathing and a productive cough for the past 2 days. During the past 6 months, he has had recurrent episodes of pneumonia treated with antibiotics. He has not gained weight in this time period. His temperature is 38.5°C (101.3°F), pulse is 130/min, respirations are 18/min, and blood pressure is 100/60 mm Hg. Auscultation of the lungs shows decreased breath sounds over the right lung fields. Ocular examination shows periorbital subcutaneous bleeding and bulging of both eyes. His leukocyte count is 16,000/mm3. An x-ray of the chest shows a right-sided opacity and a collapsed right lung. An MRI of the chest shows a heterogeneous mass in the posterior mediastinum that compresses the heart and the great vessels to the left side. Further evaluation is most likely to show which of the following?
A 9-month-old infant is brought to the pediatrician for immunizations and assessment. His parents report that he is eating well and produces several wet diapers every day. He is a happy and curious child. The boy was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. The infant's vital signs are normal. Physical growth is appropriate for his age. The physician notes a loud holosystolic murmur at the left sternal border (grade IV) and orders an echocardiogram which confirms the diagnosis of congenital heart defect. Based on echocardiogram findings, the pediatrician reassures the parents that the infant will be monitored, but most likely will not require surgical intervention. Which of the following is the most likely diagnosis?
A 7-year-old child with a history of abdominal and thigh pain that runs in his family is brought into the emergency room by his mother. His mother states they have a "blood disease." She also states the child was coughing and had fever to 101.1 F over the last three days and has been suddenly feeling much worse. On exam, the vitals are HR 110, BP 100/60, RR 20, T 101.5 F. CBC is significant for Hgb 3.2, WBC 2.1, Hct 10, Plts 30000. The reticulocyte count is 1% and the MCV is 81. Bone marrow biopsy shows hypocellular marrow with fatty tissue. What is the most likely diagnosis?
A 3-year-old boy is brought to the physician for a follow-up examination. He has suffered from seizures since the age of 8 months. His mother has noticed he often has unprovoked bouts of laughter and loves playing with water. She describes him as having a happy, excitable demeanor. He can stand without support but cannot walk. His responses are rarely verbal, and when they are, he uses single words only. His only medication is sodium valproate. He is at the 2nd percentile for head circumference, 30th percentile for height, and 60th percentile for weight. Examination shows a wide-based stance and mandibular prognathism. Tongue thrusting and difficulty standing is present. Muscle tone is increased in all extremities. Deep tendon reflexes are 4+ bilaterally. Which of the following is the mechanism most likely to explain these findings?
A 5-month-old boy is brought to the emergency department by his mother because his lips turned blue for several minutes while playing earlier that evening. She reports that he has had similar episodes during feeding that resolved quickly. He was born at term following an uncomplicated pregnancy and delivery. He is at the 25th percentile for length and below the 5th percentile for weight. His temperature is 37°C (98.6°F), pulse is 130/min, blood pressure is 83/55 mm Hg, and respirations are 42/min. Pulse oximetry on room air shows an oxygen saturation of 90%. During the examination, he sits calmly in his mother's lap. He appears well. The patient begins to cry when examination of his throat is attempted; his lips and fingers begin to turn blue. Further evaluation of this patient is most likely to show which of the following?
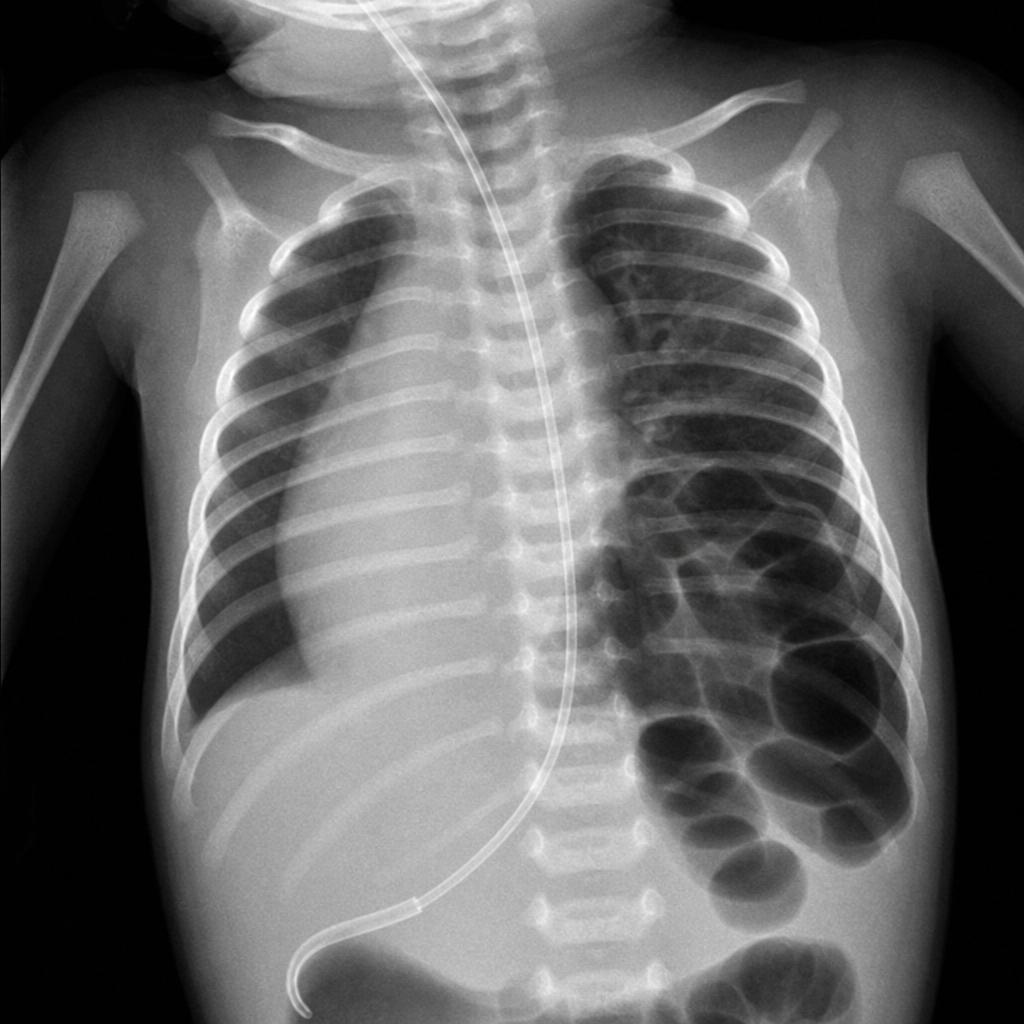
Twenty-four hours after delivery, a 2.4 kg (5.3 lb) newborn develops respiratory distress. She was born at 38 weeks gestation. The vital signs include: pulse 136/min, respiratory rate 60/min, and blood pressure 60/30 mm Hg. Examination shows a scaphoid abdomen. The heart sounds are heard in the right hemithorax, and the lung sounds are absent on the left side. The umbilical artery blood gas analysis on 60% oxygen shows: pH 7.30 pCO2 48 mm Hg pO2 52 mmHg A nasogastric tube is inserted. A chest X-ray is shown. Which of the following is the most likely diagnosis?
Practice by Chapter
Neural tube defects
Practice Questions
Congenital heart defects
Practice Questions
Gastrointestinal malformations
Practice Questions
Genitourinary anomalies
Practice Questions
Craniofacial anomalies
Practice Questions
Skeletal dysplasias
Practice Questions
Chromosomal disorders
Practice Questions
Teratogenic exposures
Practice Questions
Multiple malformation syndromes
Practice Questions
Prenatal diagnosis of congenital defects
Practice Questions
Surgical management timing
Practice Questions
Long-term outcomes and follow-up
Practice Questions
Preventive strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app