
Congenital defects — MCQs

On this page
A 2-week-old male newborn is brought to the physician because his mother has noticed her son has occasional bouts of ""turning blue in the face"" while crying. He also tires easily and sweats while feeding. He weighed 2150 g (4 lb 11 oz) at birth and has gained 200 g (7 oz). The baby appears mildly cyanotic. Examination shows a 3/6 systolic ejection murmur heard over the left upper sternal border. A single S2 is present. An echocardiography confirms the diagnosis. Which of the following factors is the main determinant of the severity of this patient's cyanosis?
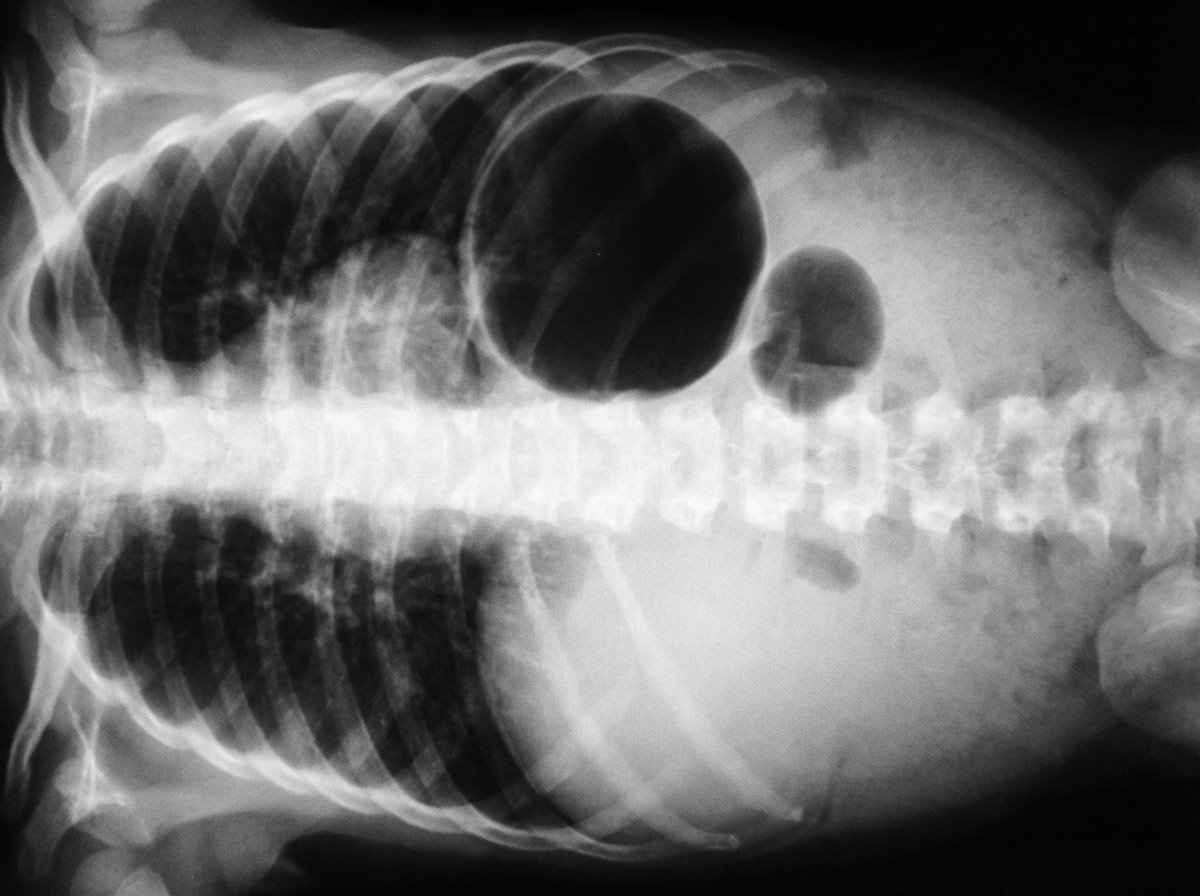
Six hours after delivery, a 3050-g (6-lb 12-oz) male newborn is noted to have feeding intolerance and several episodes of bilious vomiting. He was born at term to a healthy 35-year-old woman following a normal vaginal delivery. The pregnancy was uncomplicated, but the patient's mother had missed several of her prenatal checkups. The patient's older brother underwent surgery for pyloric stenosis as an infant. Vital signs are within normal limits. Physical examination shows epicanthus, upward slanting of the eyelids, low-set ears, and a single transverse palmar crease. The lungs are clear to auscultation. A grade 2/6 holosystolic murmur is heard at the left mid to lower sternal border. Abdominal examination shows a distended upper abdomen and a concave-shaped lower abdomen. There is no organomegaly. An x-ray of the abdomen is shown. Which of the following is the most likely diagnosis?
A 2-year-old boy is brought to the physician by his parents because of difficulty walking and cold feet for the past 2 months. His parents report that he tires quickly from walking. The patient was born at 37 weeks' gestation and has met all developmental milestones. There is no personal or family history of serious illness. He is at the 50th percentile for height and 40th percentile for weight. His temperature is 36.9°C (98.4°F), pulse is 119/min, respirations are 32/min, and blood pressure is 135/85 mm Hg. A grade 2/6 systolic murmur is heard in the left paravertebral region. Pedal pulses are absent. Further evaluation of this patient is most likely to show which of the following findings?
A 4-year-old boy is brought to his pediatrician by his mother for a physical exam before summer camp. They have no complaints or concerns at this time. He was born at 37 weeks gestation by cesarean delivery. The delivery was complicated by an omphalocele and macrosomia. During infancy and into early childhood, he struggled to breathe and eat due to an enlarged tongue. Growth and development were mostly normal with mild uneven growth of his body. He has one uncle that had similar symptoms and is alive and well. The child is up to date on all vaccines and is meeting developmental goals. He enjoys school and playing with his friends. His heart rate of 90/min, respiratory rate of 22/min, blood pressure of 110/65 mm Hg, and temperature of 36.9°C (98.4°F). Overall the child appears healthy. Physical exam findings include known hemihypertrophy of the right side along with a mildly enlarged tongue. This patient is at increased risk of developing which of the following?
A 24-hour-old girl is found to be cyanotic in the newborn nursery. She was born via spontaneous vaginal delivery at 38 weeks gestation to a gravida 1, para 0 healthy mother who received routine prenatal care. The patient is small for her gestational age. She manifests lower-extremity cyanosis along with a mesh-like mass on the back of her neck. Her vital signs are: pulse, 150/min; respirations, 48/min; and blood pressure, 120/80 mm Hg in the right arm, 124/82 mm Hg in the left arm, 80/40 mm Hg in the right leg, and 85/45 mm Hg in the left leg. Femoral pulses are 1+ and delayed. Cardiac examination shows a continuous murmur in the interscapular area. Auscultation of the lung reveals faint crackles at the base of the lung fields bilaterally. Which of the following is the most appropriate next step in management?
A two-month-old female presents to the emergency department for difficulty feeding. The patient was born at 38 weeks gestation to a 29-year-old primigravid via vaginal delivery. The newborn period has thus far been uncomplicated. The patient has been exclusively breastfed since birth. Her parents report that feeding had previously seemed to be going well, and the patient has been gaining weight appropriately. Over the past several days, the patient’s mother has noticed that the patient seems to tire out before the end of the feeding. She has also noticed that the patient begins to appear short of breath and has a bluish discoloration of her lips. The patient’s height and weight were in the 20th and 10th percentile at birth, respectively. Her current height and weight are in the 20th and 15th percentiles, respectively. Her temperature is 98.0°F (36.7°C), blood pressure is 60/48 mmHg, pulse is 143/min, and respirations are 40/min. On physical exam, the patient is in no acute distress and appears well developed. A systolic crescendo-decrescendo murmur can be heard at the left upper sternal border. Her abdomen is soft, non-tender, and non-distended. During the abdominal exam, the patient begins crying and develops cyanosis of the perioral region. Which of the following is the best initial test to diagnose this patient’s condition?
A 5-year-old boy presents to his pediatrician for a well-child visit. His mother reports him to be doing well and has no concerns. The boy was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. On physical exam, he is noted to have a right upper extremity blood pressure of 150/80 mm Hg. 2+ radial pulses and trace femoral pulses are felt. Cardiac auscultation reveals a regular rate and rhythm with a normal S1 and S2. A 2/6 long systolic murmur with systolic ejection click is heard over left sternal border and back. The point of maximal impulse is normal. Which of the following is the most likely diagnosis?
A 34-year-old G1P0 woman gives birth to a male infant at 35 weeks gestation. The child demonstrates a strong cry and moves all his arms and legs upon birth. Respirations are slow and irregular. His temperature is 99.1°F (37.3°C), blood pressure is 100/55 mmHg, pulse is 115/min, and respirations are 18/min. At a follow up appointment, the physician notices that the infant’s torso and upper extremities are pink while his lower extremities have a bluish hue. Which of the following will most likely be heard on auscultation of the patient’s chest?
A 2500-g (5-lb 8-oz) female newborn delivered at 37 weeks' gestation develops rapid breathing, grunting, and subcostal retractions shortly after birth. Despite appropriate lifesaving measures, the newborn dies 2 hours later. Autopsy shows bilateral renal agenesis. Which of the following is the most likely underlying cause of this newborn's respiratory distress?
A 2-year-old boy is brought to the physician for a well-child examination. Since infancy, he has frequently had large-volume stools that are loose and greasy. He was treated for otitis media twice in the past year. He has a history of recurrent respiratory tract infections since birth. He is at the 5th percentile for height and 3rd percentile for weight. Vital signs are within normal limits. Examination shows softening of the occipital and parietal bones. Scattered expiratory wheezing and rhonchi are heard throughout both lung fields. Which of the following is the most likely cause of this patient's symptoms?
Practice by Chapter
Neural tube defects
Practice Questions
Congenital heart defects
Practice Questions
Gastrointestinal malformations
Practice Questions
Genitourinary anomalies
Practice Questions
Craniofacial anomalies
Practice Questions
Skeletal dysplasias
Practice Questions
Chromosomal disorders
Practice Questions
Teratogenic exposures
Practice Questions
Multiple malformation syndromes
Practice Questions
Prenatal diagnosis of congenital defects
Practice Questions
Surgical management timing
Practice Questions
Long-term outcomes and follow-up
Practice Questions
Preventive strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app