
Congenital defects — MCQs

On this page
An infant boy of unknown age and medical history is dropped off in the emergency department. The infant appears lethargic and has a large protruding tongue. Although the infant exhibits signs of neglect, he is in no apparent distress. The heart rate is 70/min, the respiratory rate is 30/min, and the temperature is 35.7°C (96.2°F). Which of the following is the most likely cause of the patient’s physical exam findings?
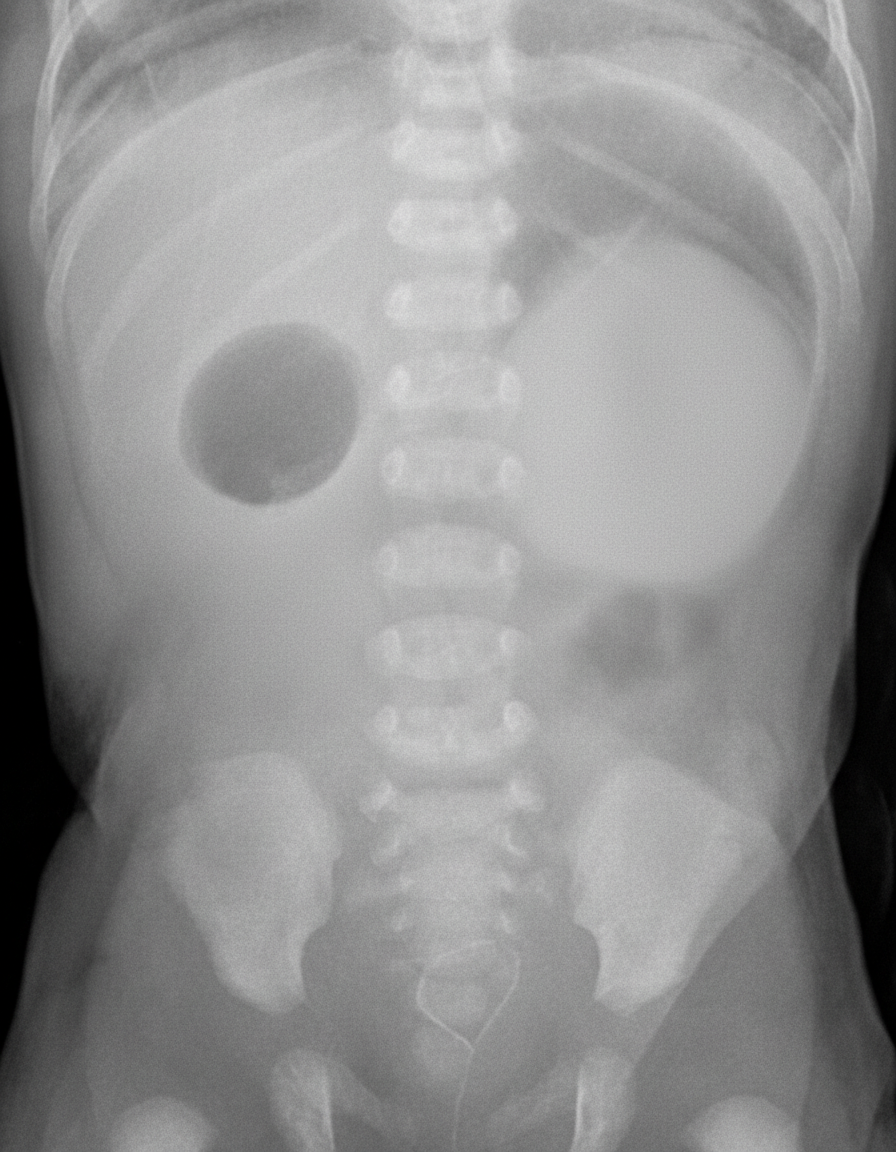
A 45-year-old gravida 1, para 0 woman is brought to the hospital in labor at 39 weeks gestation. After 4 hours, she gives birth to a healthy appearing baby boy with APGAR scores of 7 at 1 minute and 9 at 5 minutes. She had limited prenatal screening but did have an ultrasound at 35 weeks that showed polyhydramnios. The next day, the neonate vomits greenish-yellow fluid after breastfeeding. This occurs 2 more times that day after feeding and several times between feedings. The next day, the neonate appears weak with difficulty latching to the breast and is dehydrated. The physician on duty is concerned and orders blood work, IV fluids, and the abdominal X-ray shown below. Which of the following disorders is most associated with the newborn’s condition?
A 4-week-old infant is brought to the emergency department by his parents with violent vomiting. It started about 3 days ago and has slowly gotten worse. He vomits after most feedings but seems to keep some formula down. His mother notes that he is eager to feed between episodes and seems to be putting on weight. Other than an uncomplicated course of chlamydia conjunctivitis, the infant has been healthy. He was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. The physical exam is significant for a palpable mass in the right upper quadrant. What is the first-line confirmatory diagnostic test and associated finding?
A 2-day-old boy is evaluated in the newborn nursery after the nurse witnessed the child convulsing. The child was born at 39 weeks gestation to a healthy 32-year-old G1P0 woman. Initial examination after birth was notable for a cleft palate. The child’s temperature is 99°F (37.2°C), blood pressure is 100/60 mmHg, pulse is 115/min, and respirations are 18/min. On exam, he appears somnolent. His face demonstrates periorbital fullness, hypoplastic nares, and small dysmorphic ears. A series of labs are drawn and shown below: Hemoglobin: 13.1 g/dL Hematocrit: 40% Leukocyte count: 4,000/mm^3 with normal differential Platelet count: 200,000/mm^3 Serum: Na+: 140 mEq/L Cl-: 100 mEq/L K+: 3.8 mEq/L HCO3-: 25 mEq/L BUN: 19 mg/dL Glucose: 110 mg/dL Creatinine: 1.0 mg/dL Ca2+: 7.9 mg/dL Phosphate: 4.7 mg/dL This patient is deficient in a hormone that has which of the following functions?
A 2-year-old girl is brought to the physician by her parents because of clumsiness and difficulty walking. She began to walk at 12 months and continues to have difficulty standing still without support. She also appears to have difficulty grabbing objects in front of her. Over the past year, she has had 5 episodes of sinusitis requiring antibiotic treatment and was hospitalized twice for bacterial pneumonia. Physical examination shows an unstable, narrow-based gait and several hyperpigmented skin patches. Serum studies show decreased levels of IgA and IgG and an increased level of alpha-fetoprotein. Over the next 5 years, which of the following complications is this patient most likely to develop?
The medical student on the pediatric cardiology team is examining a 9-year-old girl who was referred by her primary care physician for unexplained hypertension. She is accompanied by her mother who reveals that the child is generally well but has been significantly less active than her peers for the past year. On exam, the medical student notes a thin girl in no apparent distress appearing slightly younger than stated age. Vital signs reveal a BP is 160/80, HR 80, RR 16. Physical exam is notable only for a clicking sound is noted around the time of systole but otherwise the cardiac exam is normal. Pedal pulses could not be palpated. Which of the following physical exam findings was most likely missed by both the medical student and primary care physician?
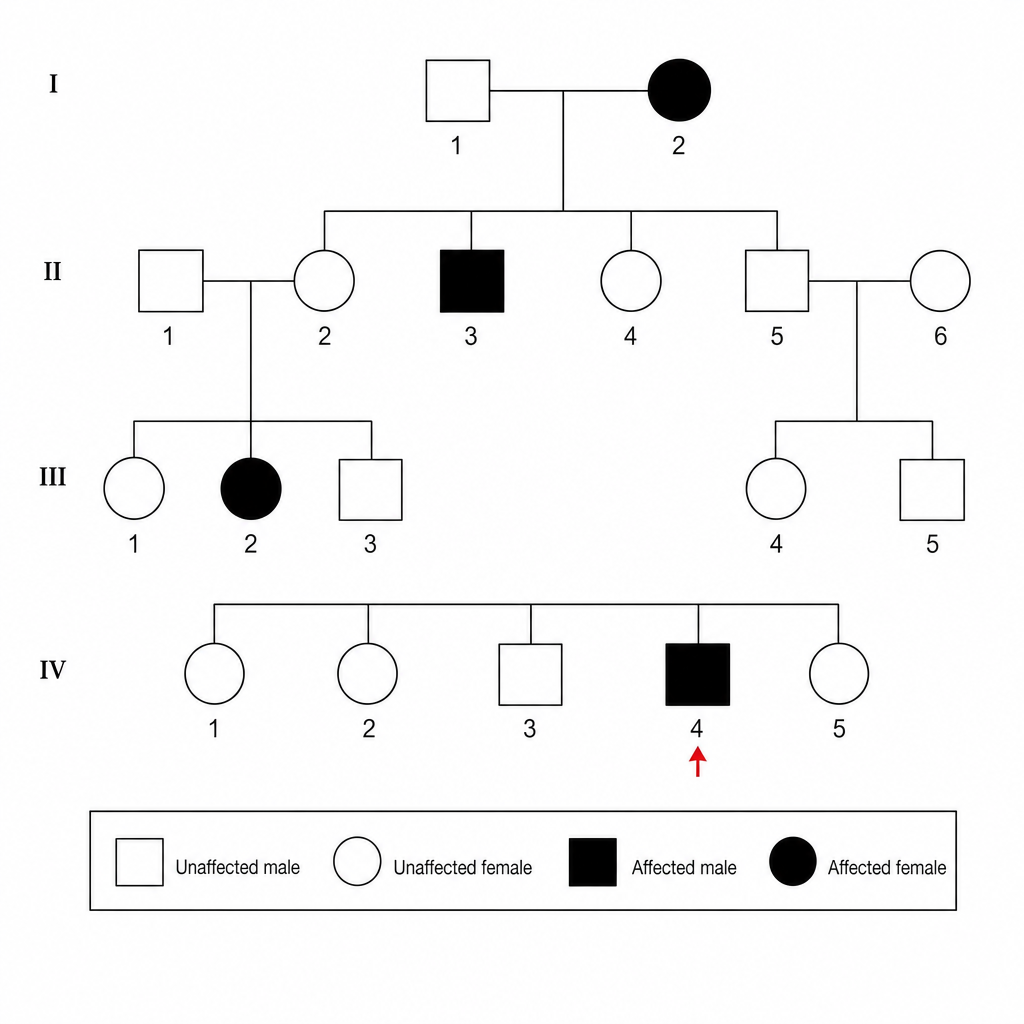
A 4-year-old boy is brought to the physician by his mother for a well-child examination. At the visit, the mother says that she is worried about the child's vision because of an “eye condition that runs in the family.” She says that the child is doing well in all activities at his preschool, except one in which he is required to sort different colored balls into baskets of a corresponding color. A pedigree chart of the family, with the patient identified by a red arrow, is shown. The most likely cause of these changes in the patient's vision involves which of the following modes of inheritance?
A 2-day old male newborn delivered vaginally at 36 weeks to a 29-year-old woman, gravida 3, para 2, has generalized convulsions lasting 2 minutes. Previous to the event, he had difficulty feeding and was lethargic. Pregnancy and delivery were uncomplicated. Apgar scores were 7 and 8 at 1 and 5 minutes, respectively. Pregnancy and delivery of the mother's first 2 children were also uncomplicated. Medications of the mother include folic acid and a multivitamin. The mother's immunizations are up-to-date. The infant appears icteric. His vital signs are within normal limits. The infant's weight and length are at the 5th percentile, and his head circumference at the 99th percentile for gestational age. There are several purpura of the skin. Ocular examination shows posterior uveitis. The patient does not pass his auditory screening tests. Cranial ultrasonography shows ventricular dilatation, as well as hyperechoic foci within the cortex, basal ganglia, and periventricular region. Which of the following is the most likely diagnosis?
A 3-year-old boy is brought to the emergency department by his mother for the evaluation of abdominal pain for one hour after drinking a bottle of toilet bowl cleaner. The mother reports that he vomited once on the way to the hospital and his vomit was non-bloody. The patient has pain with swallowing. He appears uncomfortable. Pulse oximetry shows an oxygen saturation of 82%. Examination shows heavy salivation. Oral examination shows mild oral erythema in the area of the epiglottis, but no burns. An x-ray of the chest shows no abnormalities. The patient is admitted to the intensive care unit. He is intubated and oxygenation and intravenous fluid resuscitation are begun. All contaminated clothes are removed. Which of the following is the most appropriate next step in the management of this patient?
A 10-month-old boy is brought to the clinic with a history of recurrent episodes of stridor and wheezing. His mother reports that his wheezing is exacerbated by crying, feeding, and flexion of the neck, and is relieved by extension of the neck. Occasionally he vomits after feeding. What is the most likely diagnosis?
Practice by Chapter
Neural tube defects
Practice Questions
Congenital heart defects
Practice Questions
Gastrointestinal malformations
Practice Questions
Genitourinary anomalies
Practice Questions
Craniofacial anomalies
Practice Questions
Skeletal dysplasias
Practice Questions
Chromosomal disorders
Practice Questions
Teratogenic exposures
Practice Questions
Multiple malformation syndromes
Practice Questions
Prenatal diagnosis of congenital defects
Practice Questions
Surgical management timing
Practice Questions
Long-term outcomes and follow-up
Practice Questions
Preventive strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app