
Congenital defects — MCQs

On this page
A 2800-g (6-lb 3-oz) male newborn is born at 39 weeks’ gestation to a 22-year-old woman, gravida 2, para 2, after an uncomplicated labor and delivery. The mother did not receive prenatal care. She traveled to Brazil to visit relatives during the first trimester of her pregnancy. She has bipolar disorder treated with lithium. The newborn is at the 50th percentile for height, 25th percentile for weight, and 2nd percentile for head circumference. Neurologic examination shows spasticity of the upper and lower extremities. The wrists are fixed in flexion bilaterally. Deep tendon reflexes are 4+ and symmetric. Ophthalmoscopic examination shows focal pigmentary retinal mottling. Testing for otoacoustic emissions is negative. Which of the following measures during the mother’s pregnancy is most likely to have prevented this newborn's condition?
A 4-year-old boy is brought to the pediatrician by his mother who is concerned about progressive leg weakness. His mother reports that the patient used to play outside with their neighbors for hours, but for the past few months she has seen him sitting on the sidewalk after 15 minutes because he’s too tired. The patient says his legs are “sleepy.” The patient’s mother has also had to remove the carpets from the house because the patient kept tripping over the edges. The mother reports that the patient is shy but cooperates well with his siblings and other children. He can say his first and last name and just started counting. His mother states he learned to fully walk by 15 months of age. He was hospitalized for bronchiolitis at 12 months of age, which resolved with supportive care. He had an uncomplicated orchiopexy surgery for undescended testes at 7 months of age. He has no other chronic medical conditions and takes no medications. He is up to date on his vaccinations including a flu vaccine 2 weeks ago. The patient’s mother has systemic lupus erythematous and his paternal uncle has dermatomyositis. On physical examination, bilateral calves are large in circumference compared to the thighs. Strength is 3/5 in bilateral quadriceps and 4/5 in bilateral calves. Sensation is intact. Achilles tendon reflexes are 1+ bilaterally. The patient can hop on one leg, but gets tired after 10 jumps. He has a slight waddling gait. Which of the following is the most appropriate test to confirm the diagnosis?
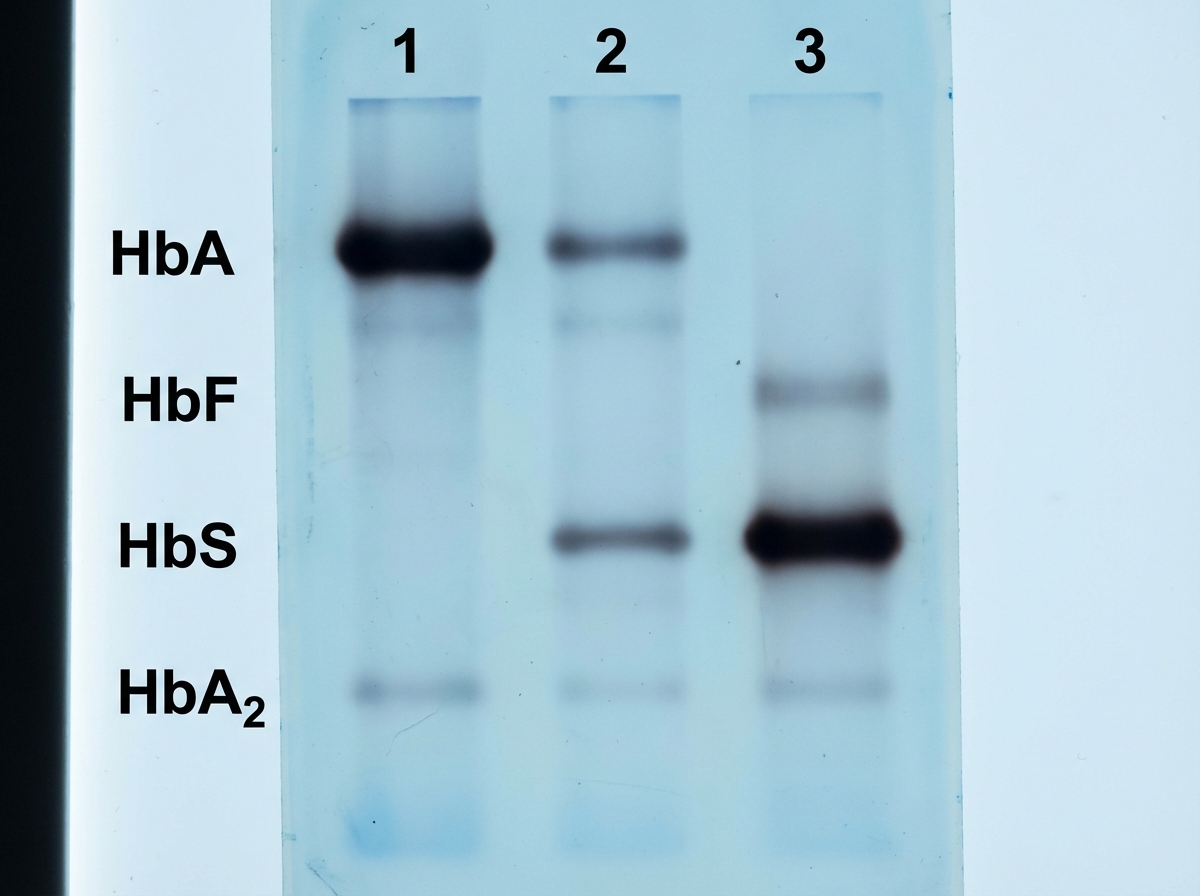
A 6-year-old African American boy presents with fever, jaundice, normochromic normocytic anemia and generalized bone pain. He has a history of similar recurrent bone pain in the past which was partially relieved by analgesics. His vital signs include: blood pressure 120/70 mm Hg, pulse 105/min, respiratory rate 40/min, temperature 37.7℃ (99.9℉), and oxygen saturation 98% in room air. On physical examination, the patient is in severe distress due to pain. He is pale, icteric and dehydrated. His abdomen is full, tense and some degree of guarding is present. Musculoskeletal examination reveals diffuse tenderness of the legs and arms. A complete blood count reveals the following: Hb 6.5g/dL Hct 18% MCV 82.3 fL Platelet 465,000/µL WBC 9800/µL Reticulocyte 7% Total bilirubin 8.4 mg/dL A peripheral blood smear shows target cells, elongated cells, and erythrocytes with nuclear remnants. Results from Hb electrophoresis are shown in the exhibit (see image). Which of the following is the most likely cause of this patient's condition?
An 11-year-old male presents to the pediatrician with his mother for evaluation of difficulty walking. His mother reports that the patient was walking normally until about a year ago, when he started to complain of weakness in his legs. He seems to be less steady on his feet than before, and he has fallen twice at home. Prior to a year ago, the patient had no difficulty walking and was active on his school’s soccer team. He has no other past medical history. The patient is an only child, and his mother denies any family history of neurological disease. On physical examination, the patient has mildly slurred speech. He has a wide-based gait with symmetric weakness and decreased sensation in his lower extremities. The patient also has the physical exam findings seen in Figures A and B. Which of the following is the most likely etiology of this patient’s presentation?

A 3-year-old is brought to the pediatrician by his mother because she is concerned about recent changes to his behavior. She states that he has seemed to regress in his motor development and has been having occasional brief episodes of uncontrollable shaking. During the subsequent work up, a muscle biopsy is obtained which demonstrates red ragged fibers and a presumptive diagnosis of a genetic disease made. The mother asks if her other son will be affected. What should be the physician's response?
A 15-year-old girl is brought to the physician because she has not yet had her first menstrual period. She reports that she frequently experiences cramping and pain in her legs during school sports. The patient is at the 20th percentile for height and 50th percentile for weight. Her temperature is 37°C (98.6°F), pulse is 70/min, and blood pressure is 155/90 mm Hg. Examination shows a high-arched palate with maloccluded teeth and a low posterior hairline. The patient has a broad chest with widely spaced nipples. Pelvic examination shows normal external female genitalia. There is scant pubic hair. Without appropriate treatment, this patient is at the greatest risk of developing which of the following complications?
A father brings his 1-year-old son into the pediatrician's office for a routine appointment. He states that his son is well but mentions that he has noticed an intermittent bulge on the right side of his son's groin whenever he cries or strains for bowel movement. Physical exam is unremarkable. The physician suspects a condition that may be caused by incomplete obliteration of the processus vaginalis. Which condition is caused by the same defective process?
A 3900-g (8.6-lb) newborn is delivered at 38 weeks' gestation to a 27-year-old woman, gravida 3, para 2, via spontaneous vaginal delivery. Immediately after delivery, he spontaneously cries, grimaces, and moves all four extremities. Over the next five minutes, he becomes cyanotic, dyspneic, and tachypneic. Mask ventilation with 100% oxygen is begun, but ten minutes after delivery the baby continues to appear cyanotic. His temperature is 37.2°C (99.0°F), pulse is 155/min, respirations are 65/min, and blood pressure is 90/60 mm Hg. Pulse oximetry on 100% oxygen mask ventilation shows an oxygen saturation of 83%. Breath sounds are normal on the right and absent on the left. Heart sounds are best heard in the right midclavicular line. The abdomen appears concave. An x-ray of the chest is shown below. Which of the following is the most appropriate initial step in the management of this patient?

A 9-year-old boy is brought to the clinic by his parents for an annual wellness examination. He is a relatively healthy boy who was born at term via vaginal delivery. He is meeting his developmental milestones and growth curves and is up-to-date on his immunizations. The father complains that he is picky with his food and would rather eat pizza. The patient denies any trouble at school, fevers, pain, or other concerns. A physical examination demonstrates a healthy boy with a grade 3 midsystolic ejection murmur at the second intercostal space that does not disappear when he sits up. What is the most likely explanation for this patient’s findings?
A 6-month-old infant is brought to the clinic for a well-child visit. The mother reports that the baby has been feeding poorly and seems to tire easily. On examination, the infant is noted to be slightly tachypneic and has a grade III/VI holosystolic murmur heard best at the left lower sternal border. Which of the following echocardiographic findings is most likely in this patient?
Practice by Chapter
Neural tube defects
Practice Questions
Congenital heart defects
Practice Questions
Gastrointestinal malformations
Practice Questions
Genitourinary anomalies
Practice Questions
Craniofacial anomalies
Practice Questions
Skeletal dysplasias
Practice Questions
Chromosomal disorders
Practice Questions
Teratogenic exposures
Practice Questions
Multiple malformation syndromes
Practice Questions
Prenatal diagnosis of congenital defects
Practice Questions
Surgical management timing
Practice Questions
Long-term outcomes and follow-up
Practice Questions
Preventive strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app