
Congenital defects — MCQs

On this page
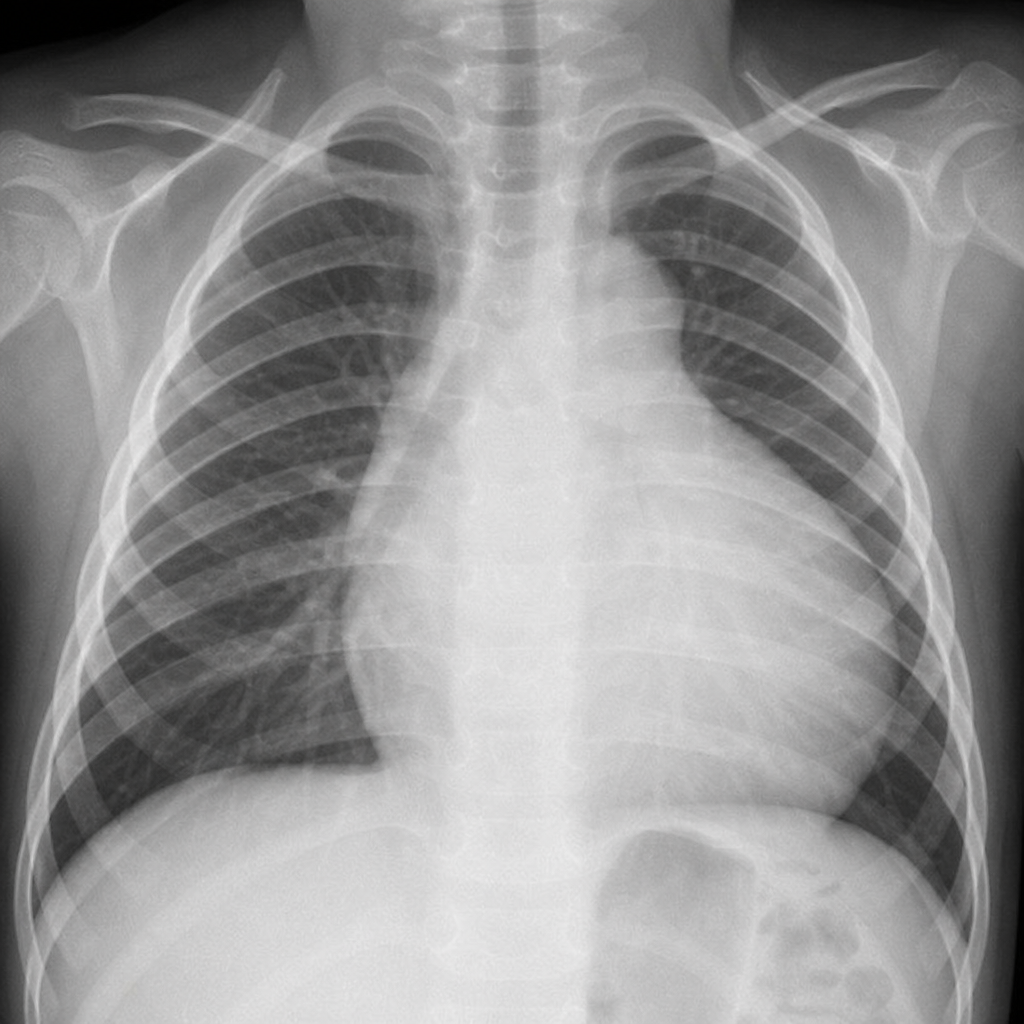
A child presents with cyanosis. Based on the chest X-ray provided, what is the most likely diagnosis?
A child presents with a webbed neck, short stature, and a low posterior hairline. What is the most likely diagnosis?
What is the characteristic metabolic finding in a baby with Congenital Hypertrophic Pyloric Stenosis (CHPS)?
A 1-year-old Caucasian male is on pancreatic enzyme replacement therapy (PERT) to maintain a healthy body mass index. Sweat chloride test is 68 mmol/L (< 29 mmol/L = normal). The patient has a relative who was also on PERT but passed away in his mid-20s due to respiratory failure, and was unable to have children. Which of the following would be most improved by PERT?
A 12-year-old boy presents to the pediatrician for a routine checkup. He and his family immigrated from Pakistan to the United States when he was 9 years of age. Per his mother, he had measles when he was 4 years of age and a high fever following a sore throat at the age 7. He received all appropriate vaccinations when he arrived in the United States. He takes no medications. He does well academically and plays soccer in a recreational league. He was born at 38 weeks gestation. His temperature is 98.4°F (36.9°C), blood pressure is 115/65 mmHg, pulse is 80/min, and respirations are 18/min. On exam, he is a healthy boy in no apparent distress. Breath sounds are equal bilaterally with good aeration. Fixed splitting of the second heart sound is noted on auscultation. Without adequate treatment, this patient will be at increased risk for developing which of the following?
An 11-year-old boy is brought to the physician for a follow-up examination. He has been having difficulties with his schoolwork over the past 4 years. He has a seizure disorder treated with valproic acid. He was able to walk independently at the age of 3 years and was able to use a fork and spoon at the age of 4 years. He is at the 40th percentile for height and 60th percentile for weight. Vitals signs are within normal limits. Examination shows multiple freckles in the axillary and groin skin folds as well as scoliosis. There are 14 hyperpigmented macules over the back and chest. There are multiple soft, painless nodules over the extremities and the trunk. Ophthalmic examination shows hyperpigmented iris nodules bilaterally. This patient is at increased risk for which of the following conditions?
A 3-week-old newborn is brought to the emergency department by his parents because of 4 episodes of vomiting that occurred that morning. The parents report that the vomit was yellowish-green with no blood in it. The patient was born at 38 weeks' gestation via vaginal delivery and has generally been healthy. He has passed normal stools each day. There is no family history of serious illness. He appears irritable and pale. His temperature is 37.0°C (98.6°F), pulse is 146/min, and blood pressure is 90/55 mm Hg. Examination shows a soft, mildly distended abdomen with no masses or organomegaly. A nasogastric tube is inserted and intravenous fluid resuscitation is initiated. An x-ray shows no gas distal to the duodenum. Which of the following is the most appropriate next step in management?
A 2-day-old female infant undergoes a newborn examination by her pediatrician. The physician adducts both of the patient's hips and exerts a posterior force on her knees; this results in an abnormally increased amount of translation of the left lower extremity in comparison to the contralateral side. The physician then abducts both hips and exerts an anterior force on the greater trochanters; this maneuver results in an audible 'clunk' heard and felt over the left hip. Ultrasound reveals decreased concavity of the left acetabulum and confirms the dislocation of the left hip when the above maneuvers are repeated under real-time ultrasound evaluation. Which of the following best characterizes this patient's condition?
A nine-year-old female presents to the pediatrician for short stature. The patient is in third grade and is the shortest child in her class. She is otherwise doing well in school, and her teacher reports that she is at or above grade level in all subjects. The patient has many friends and plays well with her two younger siblings at home. She has a past medical history of mild hearing loss in her right ear, which her previous pediatrician attributed to recurrent bouts of otitis media when she was younger. The patient’s mother is 5 feet 6 inches tall, and her father is 6 feet tall. Her family history is otherwise significant for hypothyroidism in her mother and hypertension in her father. The patient’s weight and height are in the 40th and 3rd percentile, respectively. Her temperature is 97.7°F (36.5°C), blood pressure is 155/94 mmHg, pulse is 67/min, and respirations are 14/min. On physical exam, the patient has a broad chest with widely spaced nipples. She is noted to have a short fourth metacarpal and moderate kyphosis. This patient is most likely to have which of the following findings on physical exam?
A 5-day-old boy is brought to the emergency department because of altered mental status. His mother called an ambulance after finding him grey and unarousable in his crib. The patient was born via cesarean section due to preterm premature rupture of membranes (PPROM). Since birth, the infant has gained little weight and has been generally fussy. His temperature is 37.0°C (98.6°F), the pulse is 180/min, the respirations are 80/min, the blood pressure is 50/30 mm Hg, and the oxygen saturation is 80% on room air. Physical examination shows a mottled, cyanotic infant who is unresponsive to stimulation. Cardiopulmonary examination shows prominent heart sounds, wet rales in the inferior lungs bilaterally, strong brachial pulses, and absent femoral pulses. Endotracheal intubation is performed immediately and successfully. Which of the following signs would a chest X-ray likely show?
Practice by Chapter
Neural tube defects
Practice Questions
Congenital heart defects
Practice Questions
Gastrointestinal malformations
Practice Questions
Genitourinary anomalies
Practice Questions
Craniofacial anomalies
Practice Questions
Skeletal dysplasias
Practice Questions
Chromosomal disorders
Practice Questions
Teratogenic exposures
Practice Questions
Multiple malformation syndromes
Practice Questions
Prenatal diagnosis of congenital defects
Practice Questions
Surgical management timing
Practice Questions
Long-term outcomes and follow-up
Practice Questions
Preventive strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app