
Congenital defects — MCQs

On this page
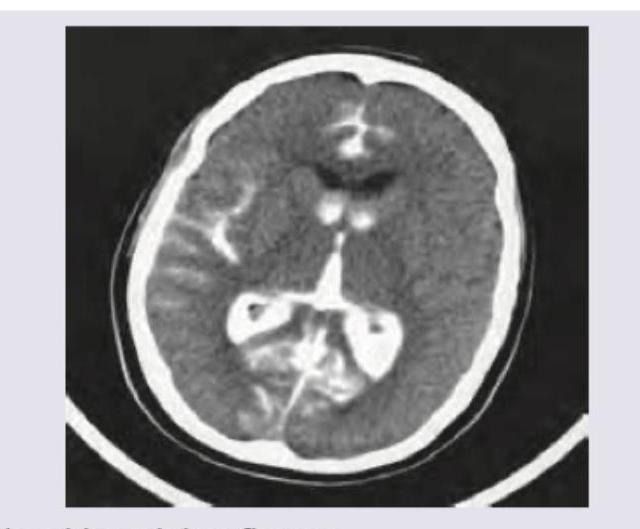
A 2-year-old boy is brought to the physician by his parents several weeks after the family immigrated from Russia. The parents are worried because the child appears to have trouble seeing and has not started walking. The child was born at home and has never been evaluated by a physician. During the pregnancy, the mother had a week of fever, myalgia, diffuse rash, and bilateral nontender cervical adenopathy after the family adopted a new cat. An MRI of the head is shown. Which of the following additional findings is most likely in this patient?
A 14-year-old boy is brought to the physician by his parents for a follow-up examination. Since early childhood, he has had recurrent respiratory infections that cause him to miss several weeks of school each year. Last month, he had received treatment for his seventh episode of sinusitis this year. He has always had bulky, foul-smelling, oily stools that are now increasing in frequency. His parents are concerned that he is too thin and not gaining weight appropriately. He has a good appetite and eats a variety of foods. He is in the 10th percentile for height and the 5th percentile for weight. Examination of the nasal cavity shows multiple nasal polyps. The lung fields are clear upon auscultation. Further evaluation is most likely to show which of the following?
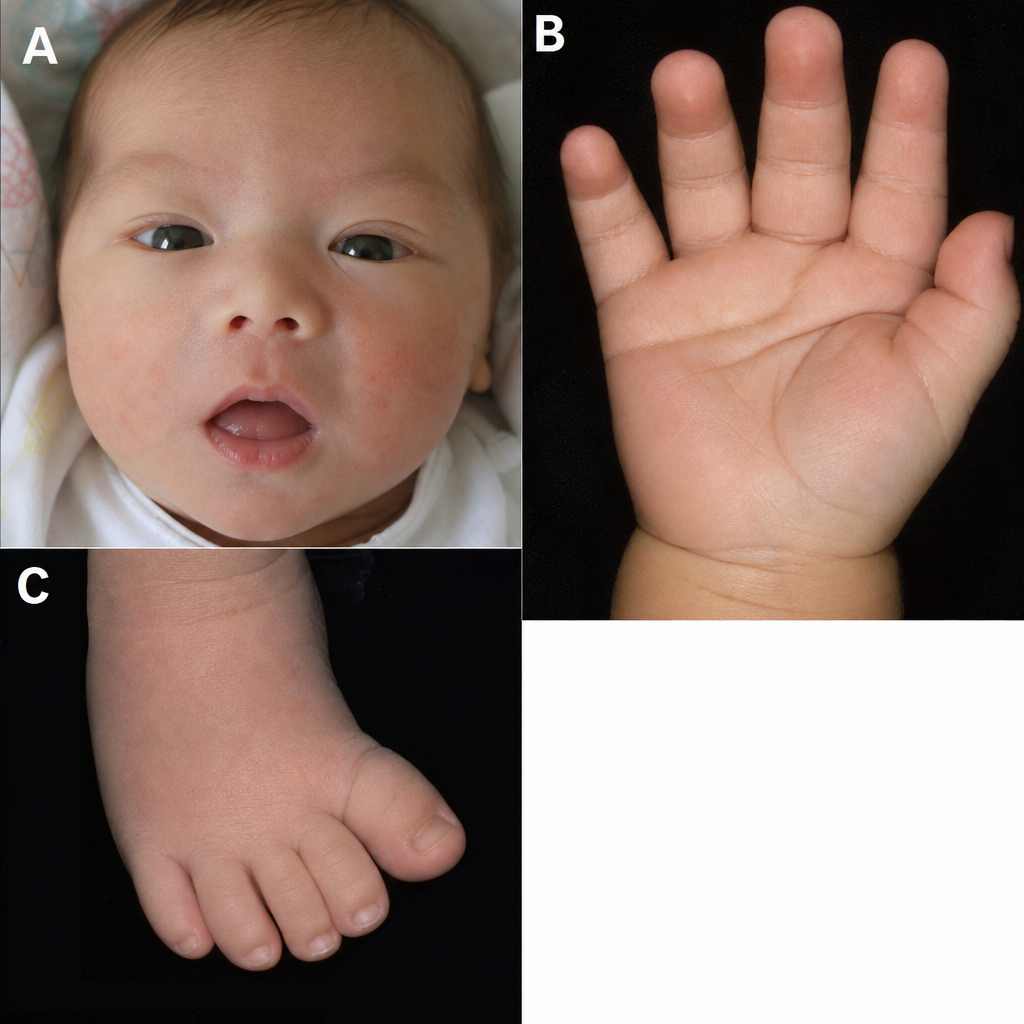
You are called to evaluate a newborn. The patient was born yesterday to a 39-year-old mother. You observe the findings illustrated in Figures A-C. What is the most likely mechanism responsible for these findings?
A 2-day-old newborn boy has failed to pass meconium after 48 hours. There is an absence of stool in the rectal vault. Family history is significant for MEN2A syndrome. Which of the following confirms the diagnosis?
A 2-year-old girl is brought to the physician by her mother for a well-child examination. Cardiac auscultation is shown. When she clenches her fist forcefully for a sustained time, the intensity of the murmur increases. Which of the following is the most likely cause of this patient's auscultation findings?
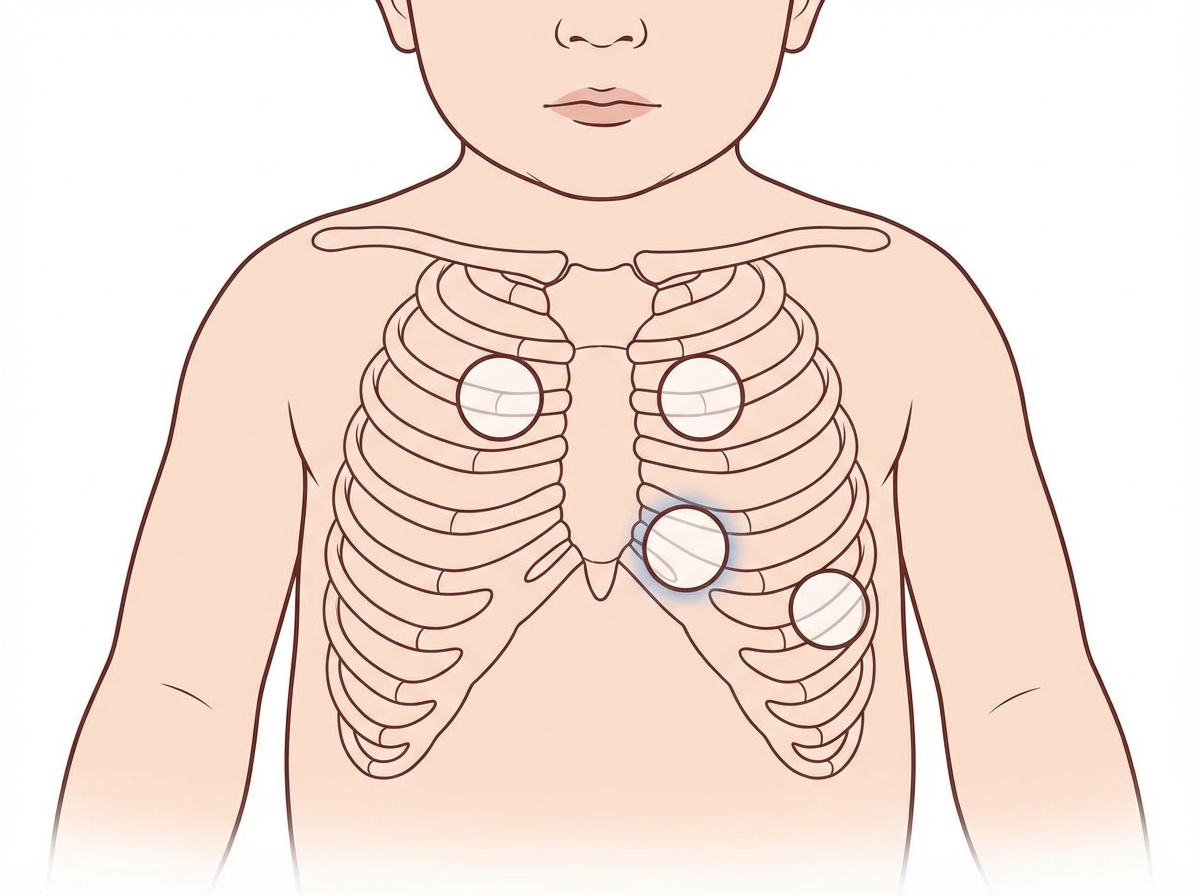
A previously healthy 2-month-old girl is brought to the emergency department because her lips turned blue while passing stools 30 minutes ago. She is at the 40th percentile for length and below the 35th percentile for weight. Pulse oximetry on room air shows an oxygen saturation of 65%, which increases to 76% on administration of 100% oxygen. Physical examination shows perioral cyanosis and retractions of the lower ribs with respiration. Cardiac examination shows a harsh grade 2/6 systolic crescendo-decrescendo murmur heard best at the left upper sternal border. Which of the following is most likely to improve this patient's symptoms?
A 5-year-old boy is brought to see his pediatrician because of painless swelling in both legs and around his eyes. His mother reports that it is worse in the morning and these symptoms have started 4 days ago. The child has just recovered from a severe upper respiratory tract infection 8 days ago. The boy was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. Today, his blood pressure is 110/65 mm Hg, the heart rate is 90/min, the respiratory rate is 22/min, and the temperature is 36.8°C (98.2°F). On physical examination, his face is edematous and there is a 2+ pitting edema over both legs up to his hips. Laboratory results are shown. Serum albumin 2.4 g/dL Serum triglycerides 250 mg/dL Serum cholesterol 300 mg/dL Urine dipstick 4+ protein Which of the following is the best initial therapy for this patient’s condition?
A 4-month-old male infant is brought in because he rejects food and is losing weight. He had several upper respiratory tract infections during the last 2 months. Upon examination, hepatosplenomegaly is noted, as well as mild hypotonia. During the next few weeks, hepatosplenomegaly progresses, the boy fails to thrive, and he continues to reject food. He has a blood pressure of 100/70 mm Hg and heart rate of 84/min. Blood tests show pancytopenia and elevated levels of transaminases. Slit lamp examination shows bilateral cherry-red spots on the macula. Chest X-ray shows a reticulonodular pattern and calcified nodules. Biopsy of the liver shows foamy histiocytes. What is the most likely diagnosis?
A 6-year-old boy is brought to the emergency department with acute intermittent umbilical abdominal pain that began that morning. The pain radiates to his right lower abdomen and occurs every 15–30 minutes. During these episodes of pain, the boy draws up his knees to the chest. The patient has had several episodes of nonbilious vomiting. He had a similar episode 3 months ago. His temperature is 37.7°C (99.86°F), pulse is 99/min, respirations are 18/min, and blood pressure is 100/60 mm Hg. Abdominal examination shows periumbilical tenderness with no masses palpated. Abdominal ultrasound shows concentric rings of bowel in transverse section. Laboratory studies show: Leukocyte Count 8,000/mm3 Hemoglobin 10.6 g/dL Hematocrit 32% Platelet Count 180,000/mm3 Serum Sodium 143 mEq/L Potassium 3.7 mEq/L Chloride 88 mEq/L Bicarbonate 28 mEq/L Urea Nitrogen 19 mg/dL Creatinine 1.3 mg/dL Which of the following is the most likely underlying cause of this patient's condition?
A pediatrician is called to examine a recently born dysmorphic boy. The birth weight was 1.6 kg (3.5 lb). On physical examination of the face and skull, the head was shown to be microcephalic with a prominent occiput and a narrow bifrontal diameter. The jaw was comparatively small with short palpebral fissures. The nose was narrow and the nasal ala was hypoplastic. Examination of the upper limbs revealed closed fists with the index fingers overlapping the 3rd fingers, and the 5th fingers overlapping the 4th fingers. The fingernails and toenails were hypoplastic and he had rocker-bottom feet. Based on these details, you suspect a particular chromosomal anomaly. Which of the following statements best describes this patient’s condition?
Practice by Chapter
Neural tube defects
Practice Questions
Congenital heart defects
Practice Questions
Gastrointestinal malformations
Practice Questions
Genitourinary anomalies
Practice Questions
Craniofacial anomalies
Practice Questions
Skeletal dysplasias
Practice Questions
Chromosomal disorders
Practice Questions
Teratogenic exposures
Practice Questions
Multiple malformation syndromes
Practice Questions
Prenatal diagnosis of congenital defects
Practice Questions
Surgical management timing
Practice Questions
Long-term outcomes and follow-up
Practice Questions
Preventive strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app