
Congenital defects — MCQs

On this page
A 5-day-old neonate is brought to the pediatrician by his parents for yellow skin for the past few days. His parents also reported that he remains quiet all day and does not even respond to sound. Further perinatal history reveals that he was born by cesarean section at 36 weeks of gestation, and his birth weight was 2.8 kg (6.1 lb). This baby is the second child of this couple, who are close relatives. Their first child died as the result of an infection at an early age. His temperature is 37.0°C (98.6°F), pulse is 116/min, and respirations are 29/min. On physical examination, hypotonia is present. His laboratory studies show: Hemoglobin 12.9 gm/dL Leukocyte count 9,300/mm3 Platelet count 170,000/mm3 Unconjugated bilirubin 33 mg/dL Conjugated bilirubin 0.9 mg/dL Coombs test Negative Which of the following is the most appropriate next step?
A 28-year-old G1P0 woman comes to the emergency department complaining that her water just broke. She reports irregular prenatal care due to her erratic schedule. She is also unsure of her gestational age but claims that her belly began to show shortly after she received her thyroidectomy for her Graves disease about 9 months ago. She denies any known fevers, chills, abnormal vaginal discharge/bleeding, or sexually transmitted infections. She develops frequent and regular contractions and subsequently goes into active labor. A fetus was later vaginally delivered with a fetal heart rate of 180 bpm. A neonatal physical examination demonstrates a lack of a sagittal cranial suture and an APGAR score of 8 and 8, at 1 and 5 minutes respectively. What findings would you expect in the baby?
A 3-year-old male is brought to the pediatrician for a check-up. The patient has a history of recurrent ear infections and several episodes of pneumonia. His mother reports the presence of scaly skin lesions on the face and in the antecubital and popliteal fossa since the patient was 2 months old. Physical examination also reveals bruising of the lower extremities and petechiae distributed evenly over the boy's entire body. A complete blood count reveals normal values except for a decreased platelet count of 45,000/mL. Which of the following findings would be expected on follow-up laboratory work-up of this patient's condition?
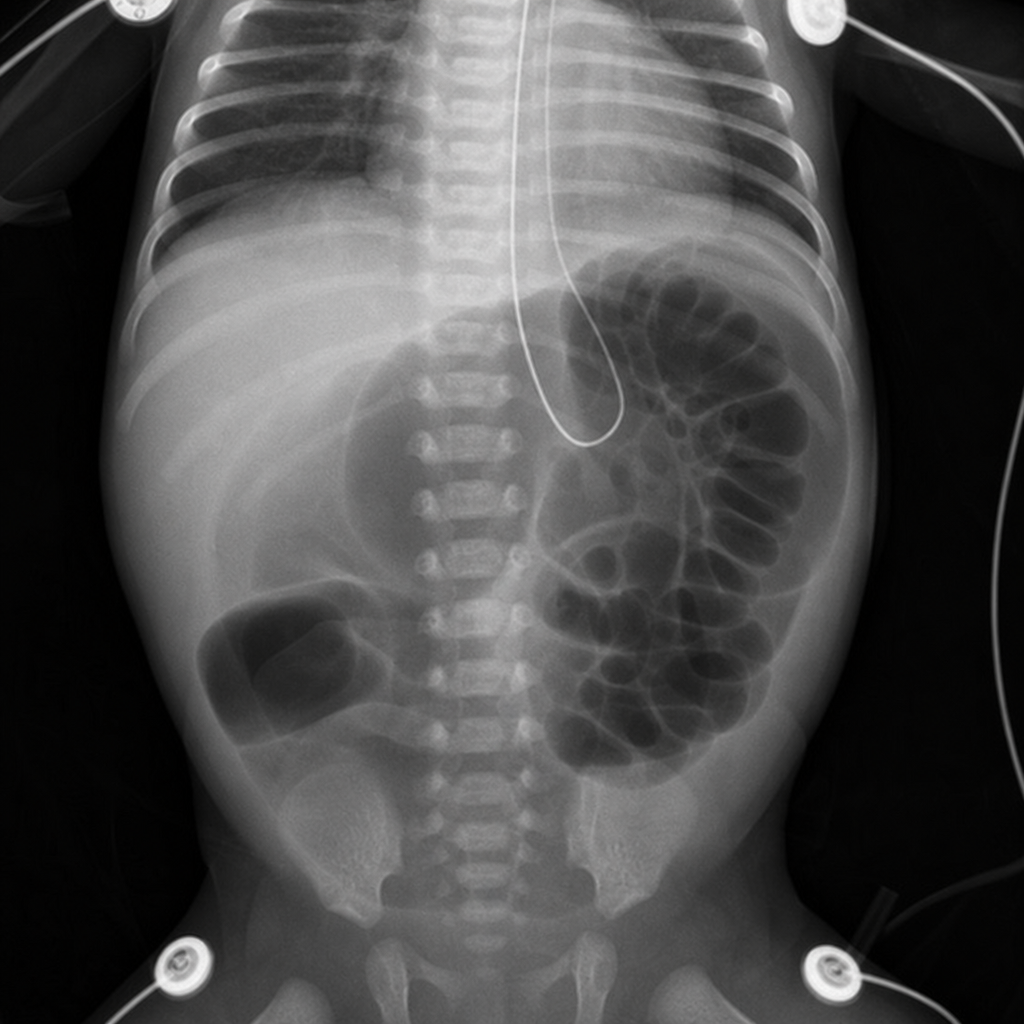
One week after delivery, a 3550-g (7-lb 13-oz) newborn has multiple episodes of bilious vomiting and abdominal distention. He passed urine 14 hours after delivery and had his first bowel movement 3 days after delivery. He was born at term to a 31-year-old woman. Pregnancy was uncomplicated and the mother received adequate prenatal care. His temperature is 37.1°C (98.8°F), pulse is 132/min, and respirations are 50/min. Examination shows a distended abdomen. Bowel sounds are hypoactive. Digital rectal examination shows a patent anus and an empty rectum. The remainder of the examination shows no abnormalities. An x-ray of the abdomen is shown. Which of the following is the underlying cause of these findings?
A 2-year-old boy is presented to the pediatrician due to poor weight gain and easy fatigability. His mother states that the patient barely engages in any physical activity as he becomes short of breath easily. The prenatal and birth histories are insignificant. Past medical history includes a few episodes of upper respiratory tract infection that were treated successfully. The patient is in the 10th percentile for weight and 40th percentile for height. The vital signs include: heart rate 122/min and respirations 32/min. Cardiac auscultation reveals clear lungs and a grade 2/6 holosystolic murmur loudest at the left lower sternal border. The remainder of the physical examination is negative for clubbing, cyanosis, and peripheral edema. Which of the following is the most likely diagnosis in this patient?
A 1-year-old boy is brought to the physician for a well-child examination. He has no history of serious illness. His older sister had an eye disease that required removal of one eye at the age of 3 years. Examination shows inward deviation of the right eye. Indirect ophthalmoscopy shows a white reflex in the right eye and a red reflex in the left eye. The patient is at increased risk for which of the following conditions?
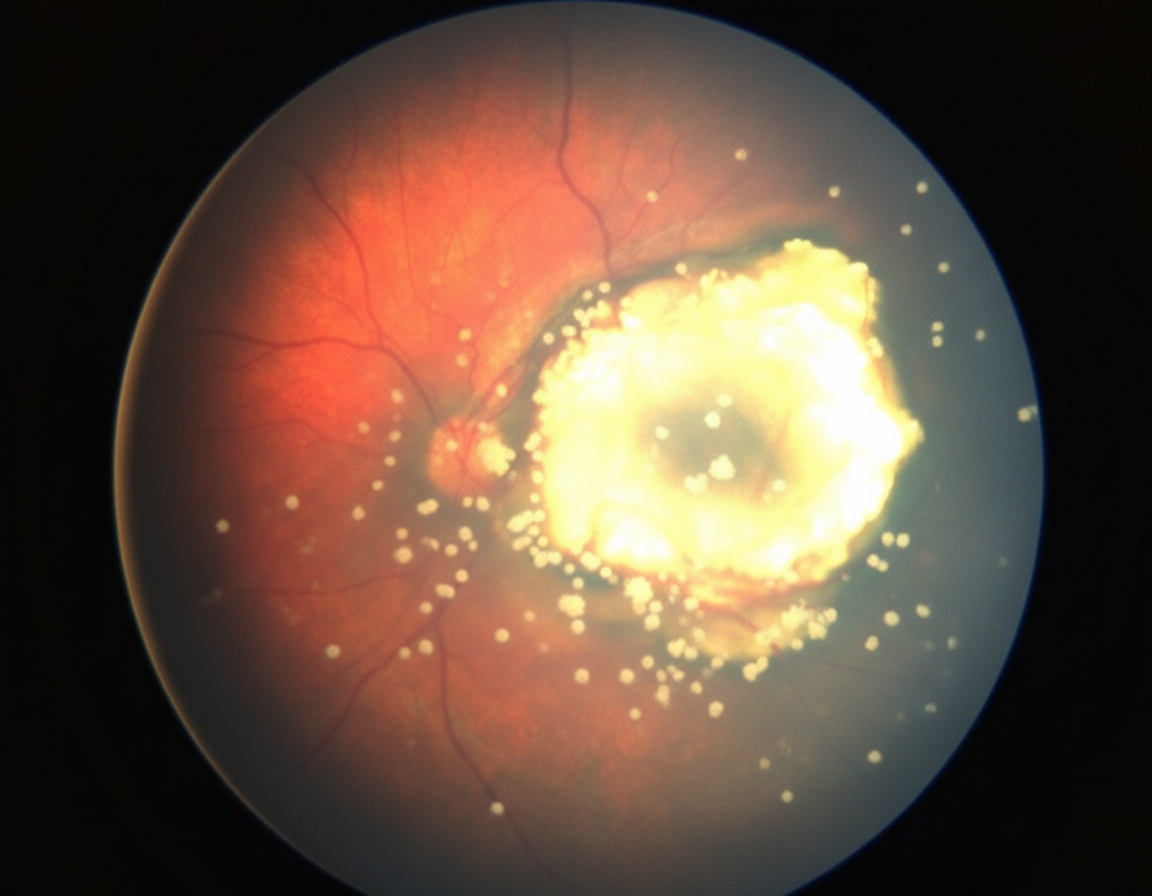
A 3-year-old boy is brought to his pediatrician for a regular checkup by his mother. The patient's mother is concerned about a slight deviation of his left eye and she also notes that her child's left eye looks strange on the photos, especially if there is a flash. The patient is the first child in the family born to a 31-year-old woman. The boy was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. Family history is unremarkable. The eye examination shows left eye converging strabismus. The pupillary reflex cannot be elicited from an illumination of the left eye. Fundal examination findings are shown in the picture. On testing, visual evoked potential cannot be elicited from the left retina but is normal from the right retina. MRI of the orbits shows a retina-derived tumor in the left eye with an initial spread along the intrabulbar part of the optic nerve and vitreous seeding. The other eye is completely intact. Which of the following methods of treatment is indicated for this patient?
A newborn girl develops poor feeding and respiratory distress 4 days after delivery. She was born at a gestational age of 29 weeks. The child was born via cesarean section due to reduced movement and a non-reassuring fetal heart tracing. APGAR scores were 6 and 8 at 1 and 5 minutes, respectively. Her vitals are as follows: Patient values Normal newborn values Blood pressure 67/39 mm Hg 64/41 mm Hg Heart rate 160/min 120–160/min Respiratory rate 60/min 40–60/min The newborn appears uncomfortable with a rapid respiratory rate and mild cyanosis of the fingers and toes. She also has nasal flaring and grunting. Her legs appear edematous. A chest X-ray shows evidence of congestive heart failure. An echocardiogram shows enlargement of the left atrium and ventricle. What medication would be appropriate to treat this infants condition?
A 2-year-old male presents to the pediatrician for abdominal pain. The patient’s parents report that he has been experiencing intermittent abdominal pain for two days. Each episode lasts several minutes, and the patient seems to be entirely well between the episodes. The pain seems to improve when the patient squats on the ground with his knees to his chest. The patient’s parents also endorse decreased appetite for two days and report that his last bowel movement was yesterday. Three days ago, the patient had two episodes of blood-streaked stools, which then seemed to resolve. His parents were not concerned at the time because the patient did not seem to be in any pain. They deny any other recent upper respiratory or gastrointestinal symptoms. The patient’s past medical history is otherwise unremarkable. His temperature is 98.2°F (36.8°C), blood pressure is 71/53 mmHg, pulse is 129/min, and respirations are 18/min. The patient is happily playing in his mother’s lap. His abdomen is soft and non-distended, and he is diffusely tender to palpation over the entire right side. A 2x4 cm cylindrical mass can be palpated in the right upper quadrant. Which of the following is most likely to be found in this patient?
A 7-year-old boy is brought to the pediatrician by his parents for a routine checkup. The parents note that the patient recently joined a baseball team and has had trouble keeping up with his teammates and gets short of breath with exertion. The patient has otherwise been healthy and has no known history of asthma or allergic reaction. Today, the patient’s temperature is 98.2°F (36.8°C), blood pressure is 112/72 mmHg, pulse is 70/min, and respirations are 12/min. The physical exam is notable for a heart murmur that decreases when the patient bears down. Additionally, the hand grip and rapid squatting maneuvers increase the severity of the murmur. Which of the following is likely heard on auscultation?
Practice by Chapter
Neural tube defects
Practice Questions
Congenital heart defects
Practice Questions
Gastrointestinal malformations
Practice Questions
Genitourinary anomalies
Practice Questions
Craniofacial anomalies
Practice Questions
Skeletal dysplasias
Practice Questions
Chromosomal disorders
Practice Questions
Teratogenic exposures
Practice Questions
Multiple malformation syndromes
Practice Questions
Prenatal diagnosis of congenital defects
Practice Questions
Surgical management timing
Practice Questions
Long-term outcomes and follow-up
Practice Questions
Preventive strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app