
Congenital defects — MCQs

On this page
An 8-year-old girl is brought to the physician by her parents for the evaluation of an episode of unconsciousness while at the playground that morning. She was unconscious for about 15 seconds and did not shake, bite her tongue, or lose bowel or bladder control. Her grandfather died suddenly at the age of 29 of an unknown heart condition; her parents are both healthy. An ECG shows sinus rhythm and a QT interval corrected for heart rate (QTc) of 470 milliseconds. Laboratory studies are within normal limits. Which of the following is the most likely additional finding in this patient?
A 2-year-old boy is brought to the emergency department after his mother noticed maroon-colored stools in his diaper. He has not had any diarrhea or vomiting. The prenatal and birth histories are unremarkable, and he has had no recent trauma. He tolerates solid foods well. The vital signs include: temperature 37.0℃ (98.6℉), blood pressure 90/60 mm Hg, pulse 102/min, and respiratory rate 16/min. The weight is at the 50th percentile. The examination revealed an alert boy with pallor. The abdomen was mildly tender at the right iliac region without masses. There were no anal fissures or hemorrhoids. A stool guaiac test was positive. The laboratory results are as follows: Complete blood count (CBC) Leukocytes 7,500/uL Hemoglobin 9 g/dL Hematocrit 24% Platelets 200,000/uL Which of the following is the most appropriate next step in the management of this patient?
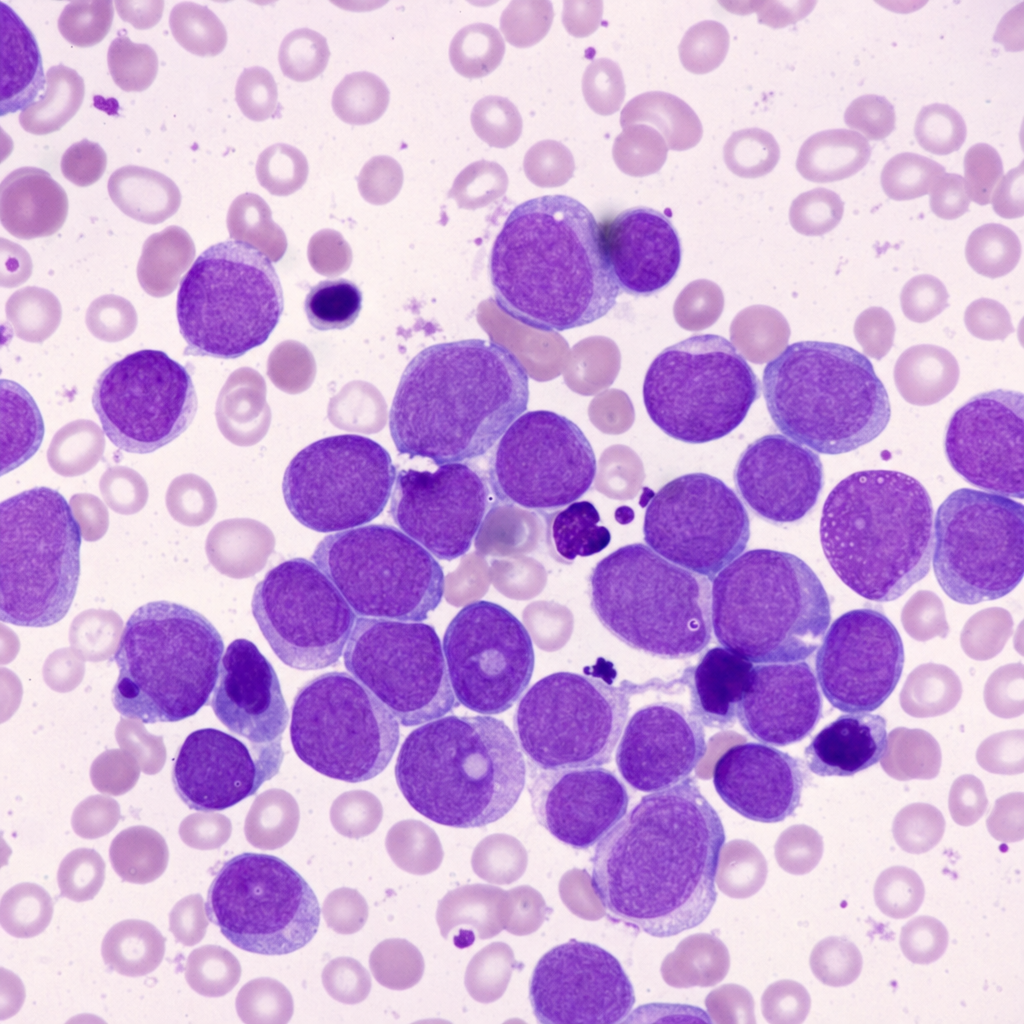
A 2-month-old baby boy and his mother present to his pediatrician for vaccination as per the immunization schedule. His mother denies any active complaints but mentions that he has not smiled yet. The boy was born at 39 weeks gestation via spontaneous vaginal delivery. His mother received minimal prenatal care. On physical examination, his vitals are stable, but a general examination shows the presence of generalized hypotonia. His face is characterized by upwardly slanting palpebral fissures, small dysplastic ears, and a flat face. His little fingers are short, with clinodactyly, and both palms have single palmar creases. The results of a karyotype are shown in the image. If this infant has also acquired a somatic mutation in the GATA1 gene, for which of the following conditions is he most likely to be at increased risk?
An 8-year-old girl is brought to the physician for a well-child examination. Since the age of 2 years, she has had multiple fractures after minor trauma. During the past year, she has fractured the left humerus and right clavicle after falls. Her father also has a history of recurrent fractures. She is at the 5th percentile for height and 20th percentile for weight. Vital signs are within normal limits. Physical examination shows increased convexity of the thoracic spine. Forward bend test demonstrates asymmetry of the thoracolumbar region. There is a curvature of the tibias bilaterally, and the left leg is 2 cm longer than the right. There is increased mobility of the joints of the upper and lower extremities. Which of the following is the most likely additional finding?
A 5-year-old boy is brought to the emergency department by his stepmother because of multiple injuries. She says that he sustained these injuries while playing. Radiographic findings show multiple fractures in various stages of healing. Physical examination shows the findings in the image below. What is the most likely diagnosis in this patient?

A 25-year-old woman, gravida 2, para 1, at 36 weeks' gestation comes to the physician because of irritability, palpitations, heat intolerance, and frequent bowel movements for the last 5 months. She has received no prenatal care. Her pulse is 118/min and blood pressure is 133/80 mm Hg. She appears anxious. There is a fine tremor in the hands and ophthalmologic examination shows bilateral exophthalmos. The skin is warm and moist to touch. This patient's child is at risk for which of the following complications at birth?
A 45-day-old male infant is brought to a pediatrician by his parents with concerns of poor feeding and excessive perspiration for one week. On physical examination, his temperature is 37.7°C (99.8°F), pulse rate is 190/min, and respiratory rate is 70/min. Mild cyanosis is present over the lips, and over the nail beds. Oxygen is provided and his oxygen saturation is carefully monitored. The pediatrician orders a bedside echocardiogram of the infant. It reveals a single arterial trunk arising from 2 normally formed ventricles. The arterial trunk is separated from the ventricles by a single semilunar valve. There is a defect in the interventricular septum, and the arterial trunk overrides the defect. Which of the following congenital heart diseases can also present with similar clinical features?
A 4-hour-old male newborn has perioral discoloration for the past several minutes. Oxygen by nasal cannula does not improve the cyanosis. He was delivered by cesarean delivery at 37 weeks' gestation to a 38-year-old woman, gravida 3, para 2. Apgar scores were 8 and 9 at 1 and 5 minutes, respectively. The mother has type 2 diabetes mellitus that was well-controlled during the pregnancy. She has not received any immunizations since her childhood. The newborn's temperature is 37.1°C (98.8°F), pulse is 170/min, respirations are 55/min, and blood pressure is 80/60 mm Hg. Pulse oximetry shows an oxygen saturation of 85%. Cardiopulmonary examination shows a 2/6 holosystolic murmur along the lower left sternal border. The abdomen is soft and non-tender. Echocardiography shows pulmonary arteries arising from the posterior left ventricle, and the aorta rising anteriorly from the right ventricle. Which of the following is the most appropriate next step in the management of this patient?
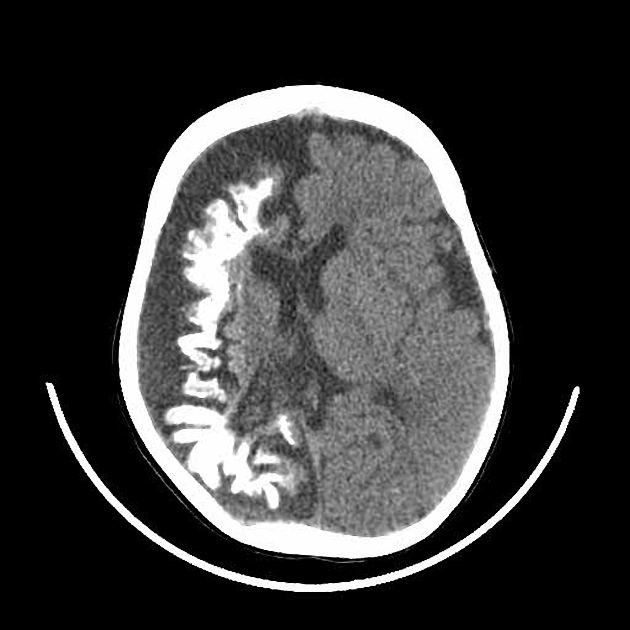
A 10-year-old boy is brought to a family physician by his mother with a history of recurrent headaches. The headaches are moderate-to-severe in intensity, unilateral, mostly affecting the right side, and pulsatile in nature. Past medical history is significant for mild intellectual disability and complex partial seizures that sometimes progress to secondary generalized seizures. He was adopted at the age of 7 days. His birth history and family history are not available. His developmental milestones were slightly delayed. There is no history of fever or head trauma. His vital signs are within normal limits. His height and weight are at the 67th and 54th percentile for his age. Physical examination reveals an area of bluish discoloration on his right eyelid and cheek. The rest of the examination is within normal limits. A computed tomography (CT) scan of his head is shown in the exhibit. Which of the following additional clinical findings is most likely to be present?
A 1-week-old baby is brought to the pediatrician’s office for a routine checkup. On examination, she is observed to have microcephaly with a prominent occiput. She also has clenched fists and rocker-bottom feet with prominent calcanei. A cardiac murmur is evident on auscultation. Based on the clinical findings, a diagnosis of nondisjunction of chromosome 18 is suspected. The pediatrician orders a karyotype for confirmation. He goes on to explain to the mother that her child will face severe growth difficulties. Even if her daughter progresses beyond a few months, she will not be able to reach developmental milestones at the appropriate age. In addition to the above, which of the following is most likely a consequence of this genetic disturbance?
Practice by Chapter
Neural tube defects
Practice Questions
Congenital heart defects
Practice Questions
Gastrointestinal malformations
Practice Questions
Genitourinary anomalies
Practice Questions
Craniofacial anomalies
Practice Questions
Skeletal dysplasias
Practice Questions
Chromosomal disorders
Practice Questions
Teratogenic exposures
Practice Questions
Multiple malformation syndromes
Practice Questions
Prenatal diagnosis of congenital defects
Practice Questions
Surgical management timing
Practice Questions
Long-term outcomes and follow-up
Practice Questions
Preventive strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app