
Congenital defects — MCQs

On this page
A 31-year-old woman delivers a healthy boy at 38 weeks gestation. The delivery is vaginal and uncomplicated. The pregnancy was unremarkable. On examination of the newborn, it is noted that his head is tilted to the left and his chin is rotated to the right. Palpation reveals no masses or infiltration in the neck. The baby also shows signs of left hip dysplasia. Nevertheless, the baby is active and exhibits no signs of other pathology. What is the most probable cause of this patient's condition?
Over the course of a year, 5 children with identical congenital heart defects were referred to a pediatric cardiac surgeon for evaluation. All 5 children had stable vital signs and were on appropriate medication. Upon review of medical records, all of them had a loud holosystolic murmur over the third intercostal space at the left sternal border. The surgeon ordered echocardiograms for all 5 children and recommended surgical closure of the defect in one of them. Which of the following patients required surgical repair of their defect?
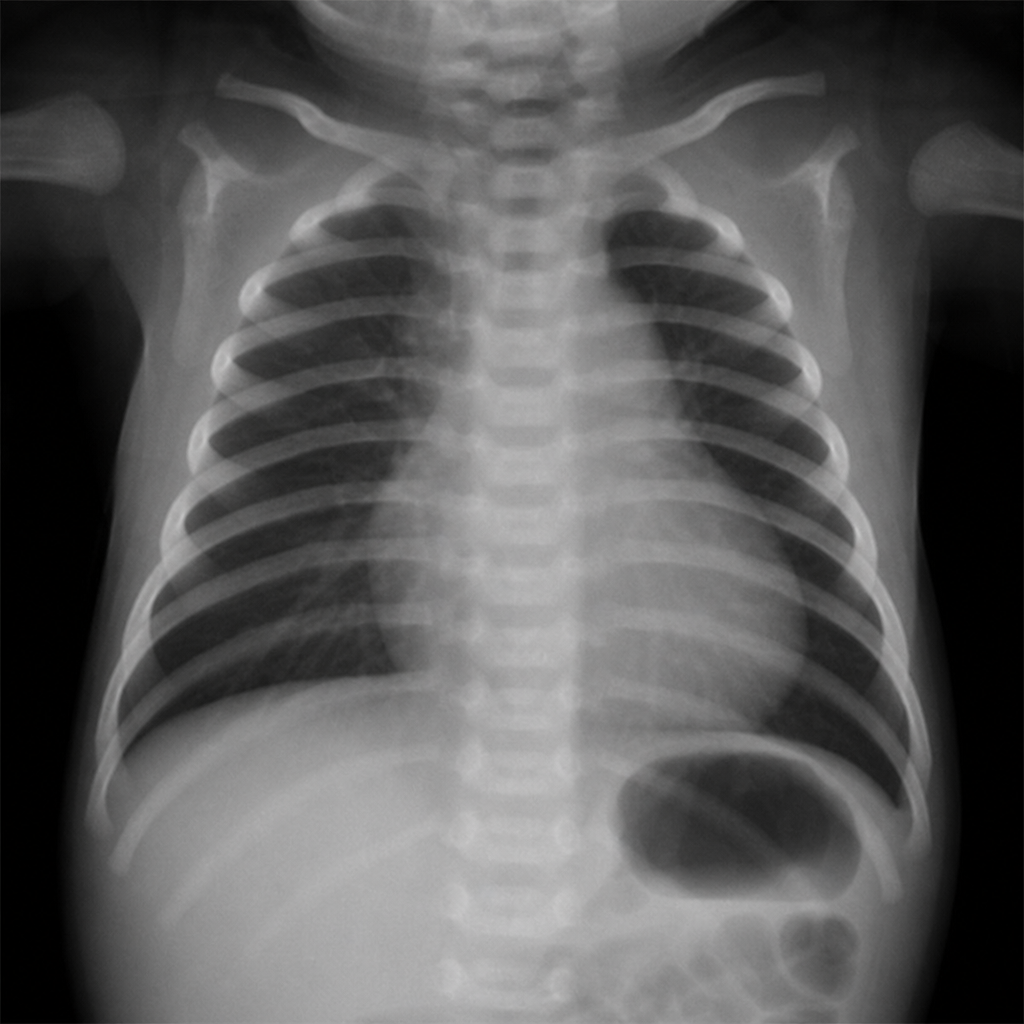
A 5-year-old child has central cyanosis and episodes of worsening cyanosis during exertion that improve when he squats. Examination shows digital clubbing, a right ventricular heave, a single S2, and a harsh systolic ejection murmur at the left upper sternal border. The chest radiograph shown was obtained during an unrelated evaluation of enteric tubing; it shows no pulmonary edema or focal lung disease. Which congenital heart defect most likely explains the child's clinical findings?
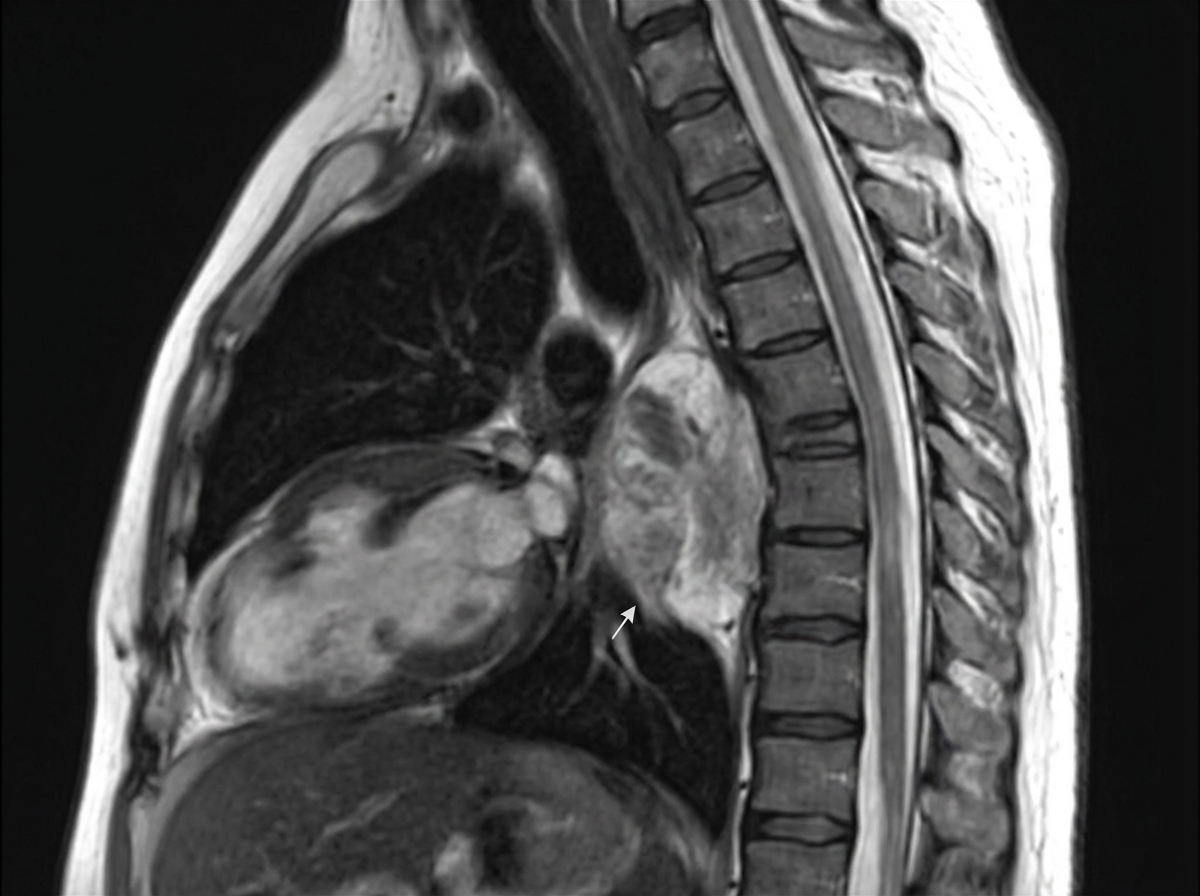
A 7-year-old girl presents with a lump in her neck which she noticed a few days ago. The patient's mother states that her daughter's left eyelid seems to be drooping, making her left eye look small. There is no significant past medical history. On neurological examination, the patient has normal bilateral pupillary reflexes but a miotic left pupil. A lateral radiograph of the chest reveals a mass in the posterior mediastinum with no evidence of bone erosion. An MRI is performed and the results are shown in the image. An imaging-guided biopsy of the mass reveals spindle-shaped cells arranged chaotically, with moderate cytoplasm and small nuclei. Scattered mature ganglion cells with abundant cytoplasm and round to oval nuclei are also present. In addition, there are nests of small, round, immature neuroblasts with hyperchromatic nuclei and scant cytoplasm, consistent with a neuroblastomatous component. The overall findings are consistent with ganglioneuroblastoma. The biopsy tissue is analyzed with immunohistochemistry and found to be positive for S-100, synaptophysin, and chromogranin. Which of the following factors is associated with poor prognosis for this patient's most likely diagnosis?
A 1-month-old girl is brought to the physician for a follow-up examination. The mother has noticed that the girl's neck is always tilted to the right. She was delivered at term, and childbirth was complicated by a breech position. There is no family history of serious illness. She appears healthy. She is at 60th percentile for length and weight. Her temperature is 37.1°C (98.8°F), pulse is 102/min, and respirations are 42/min. Examination shows the head tilted toward the right, and the chin rotated towards the left. Range of motion of the neck is limited. There is a palpable, firm, well-circumscribed mass in the right lower side of the neck. The remainder of the examination shows no abnormalities. Which of the following is the most appropriate next best step in management?
A 4-month-old is noted to have a grade 3/6, harsh, systolic ejection murmur heard at the left upper sternal border. The mother reports that the child's lips occasionally turn blue during feeding. A cardiologist recommends surgery. Later, the physician remarks that the infant's congenital abnormality was related to a failure of neural crest cell migration. Prior to surgery, which of the following was a likely finding?
A 10-month-old boy is being treated for a rare kind of anemia and is currently being evaluated for a bone marrow transplant. The patient’s mother presents to an appointment with their pediatrician after having done some online research. She has learned that the majority of patients inherit this condition as an autosomal dominant mutation. As a result of the genetic mutation, there is impaired erythropoiesis, leading to macrocytic red blood cells without hypersegmented neutrophils. She also read that children who survive will eventually present with short stature and craniofacial abnormalities. Which of the following is true about this patient’s condition?
A 1-year-old boy presents to pediatrics clinic for a well-child visit. He has no complaints. He has a cleft palate and an abnormal facial appearance. He has been riddled with recurrent infections and is followed by cardiology for a ventricular septal defect (VSD). Vital signs are stable, and the patient's physical exam is benign. If this patient's medical history is part of a larger syndrome, what might one also discover that is consistent with the manifestations of this syndrome?
A 3-month-old boy is brought to the physician by his mother because of poor weight gain. She also reports a dusky blue discoloration to his skin during feedings and when crying. On examination, there is a harsh, systolic murmur heard over the left upper sternal border. An x-ray of the chest shows a boot-shaped heart. Which of the following is the most likely cause of his symptoms?
A 5-year-old boy with Down syndrome presents with his mother. The patient's mother says that he isn't playing or eating as much as he used to and seems lethargic. She also reports that he has had chronic constipation since infancy and has never had a normal bowel movement without intervention. Expected developmental delays are present and stable. Physical examination reveals dry mucous membranes and abdominal distention with no tenderness to palpation. An abdominal radiograph is shown in the image below. Which of the following is the most likely diagnosis in this patient?

Practice by Chapter
Neural tube defects
Practice Questions
Congenital heart defects
Practice Questions
Gastrointestinal malformations
Practice Questions
Genitourinary anomalies
Practice Questions
Craniofacial anomalies
Practice Questions
Skeletal dysplasias
Practice Questions
Chromosomal disorders
Practice Questions
Teratogenic exposures
Practice Questions
Multiple malformation syndromes
Practice Questions
Prenatal diagnosis of congenital defects
Practice Questions
Surgical management timing
Practice Questions
Long-term outcomes and follow-up
Practice Questions
Preventive strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app