
Congenital defects — MCQs

On this page
A 12-day-old male newborn is brought to the emergency department because of a high-grade fever for 3 days. He has been lethargic and not feeding well during this period. He cries incessantly while passing urine. There is no family history of serious illness. He was delivered at 37 weeks' gestation and pregnancy was complicated by mild oligohydramnios. His immunizations are up-to-date. He is at the 35th percentile for length and 40th percentile for weight. His temperature is 39°C (102.2°F), pulse is 165/min, respirations are 60/min, and blood pressure is 55/30 mm Hg. Examination shows open anterior and posterior fontanelles. There is a midline lower abdominal mass extending 2–3 cm above the symphysis. Cardiopulmonary examination shows no abnormalities. The child is diagnosed with a urinary tract infection and broad spectrum antibiotic therapy is begun. This patient will most likely benefit the most from which of the following interventions?
A 2-year-old boy is brought to the physician by his parents for a well-child visit. During his last well-child visit 9 months ago, the patient had not begun talking. The parents report that their son frequently avoids eye contact and has no friends at daycare. He was born at term and has been healthy except for an episode of otitis media 6 months ago, which was treated with amoxicillin. His immunizations are up-to-date. He is at the 95 percentile for height, 20 percentile for weight, and 95 percentile for head circumference. He appears shy. His temperature is 37°C (98.6°F), pulse is 120/min, and blood pressure is 100/55 mm Hg. Examination shows elongated facial features and large ears. The patient does not speak. He does not follow instruction to build a stack of 2 blocks. Throughout the examination, he continually opens and closes his mother's purse and does not maintain eye contact. Which of the following findings is most likely to confirm the diagnosis?
A 14-year-old girl is brought to the physician because she frequently experiences cramping and pain in her legs during school sports. She is at the 10th percentile for height. Her blood pressure is 155/90 mm Hg. Examination shows a high-arched palate with maloccluded teeth and a low posterior hairline. The patient has a broad chest with widely spaced nipples. Pelvic examination shows normal external female genitalia with scant pubic hair. Without appropriate treatment, this patient is at the greatest risk of developing which of the following complications?
A 4-year-old male is brought into your office because his mother states he has been fatigued. He has not been acting like himself and has been getting tired easily while running around and playing with other children. As of last week, he has also been complaining of being short of breath. His vitals are temperature 98.6 deg F (37.2 deg C), blood pressure 100/75 mmHg, pulse 98/min, and respirations 22/min. On exam, the patient is short of breath, and there is a holosystolic murmur with an appreciable thrill along the left sternal border. There are no other noticeable abnormalities, and the mother states that the child's prenatal course along with genetic testing was normal. What is the most likely diagnosis?
A 2720-g (6-lb) female newborn delivered at 35 weeks’ gestation starts vomiting and becomes inconsolable 48 hours after birth. The newborn has not passed her first stool yet. Examination shows abdominal distention and high-pitched bowel sounds. A water-soluble contrast enema study shows microcolon. Serum studies show increased levels of immunoreactive trypsinogen. Which of the following is the most likely additional laboratory finding?
A 13-month-old girl is brought to the pediatric clinic by her mother due to progressive abdominal distension, poor feeding, and failure to thrive. The perinatal history was uneventful. The family emigrated from Sudan 8 years ago. The vital signs include: temperature 36.8°C (98.2°F), blood pressure 100/55 mm Hg, and pulse 99/min. The physical examination shows conjunctival pallor, hepatosplenomegaly, and parietal and frontal bossing of the skull. The laboratory test results are as follows: Hemoglobin 8.7 g/dL Mean corpuscular volume 62 μm3 Red cell distribution width 12.2% (normal value is 11.5–14.5%) Reticulocyte count 2.1 % Leucocyte count 10,200/mm3 Platelet count 392,000/mm3 The peripheral blood smear shows microcytic red cells, target cells, and many nucleated red cells. Which of the following is the most likely diagnosis?
A 2-year-old boy is brought to the physician because of an increasing productive cough with a moderate amount of white phlegm for the past week. He has been treated for pneumonia with antibiotic therapy four times over the past year. A chest x-ray performed 3 months ago showed no anatomical abnormalities. He has had multiple episodes of bulky greasy stools that don't flush easily. He is at 3rd percentile for height and at 5th percentile for weight. His temperature is 38°C (100.4°F), pulse is 132/min, and respirations are 44/min. A few inspiratory crackles are heard in the thorax. The abdomen is soft and nontender. The remainder of the examination shows no abnormalities. Which of the following is the best initial test to determine the underlying etiology of this patient's illness?
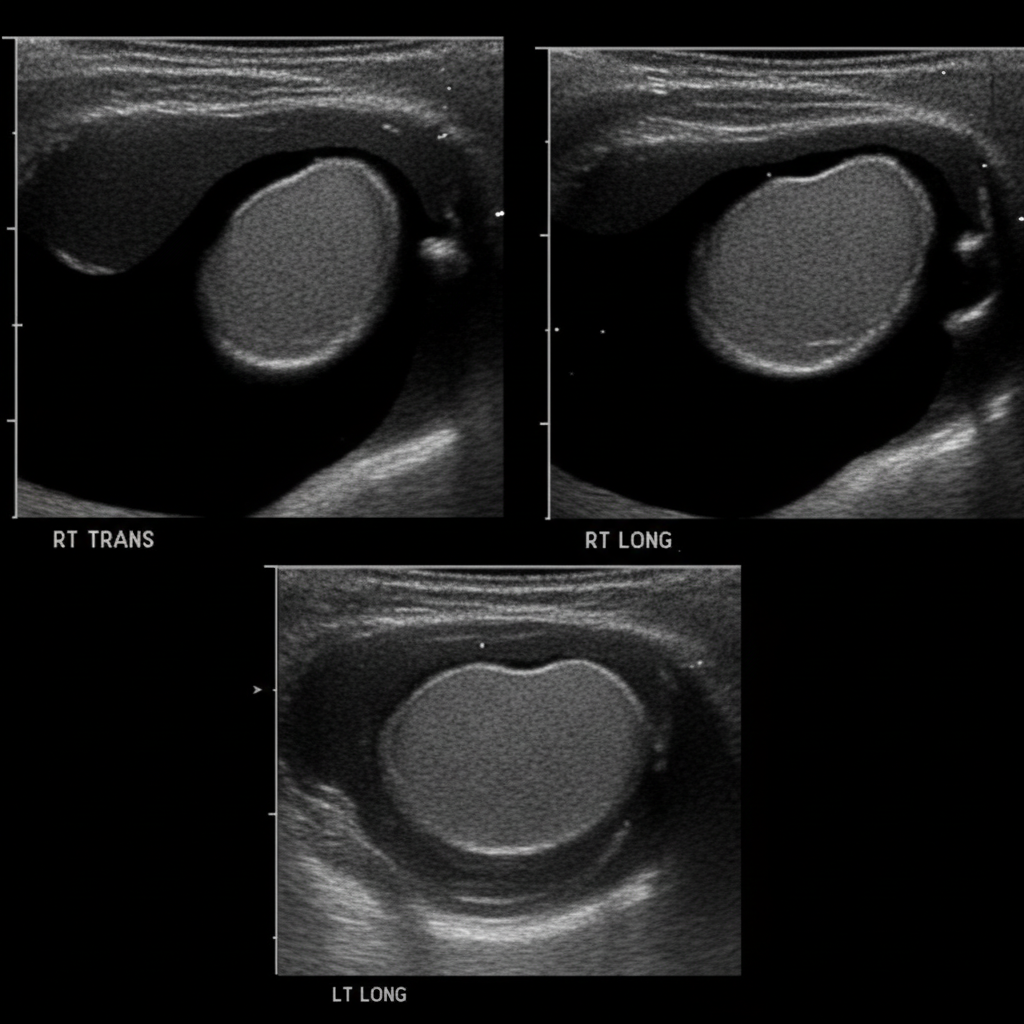
A 5-year-old boy is taken to his pediatrician by his mother for evaluation of painless testicular swelling. His mother says that it became apparent at 1 year of age and has been progressively increasing in size. There is no history of infectious diseases other than the seasonal flu. The boy has no history of trauma or surgery. He has not visited any tropical countries and his vaccinations are up to date. The vital signs are normal for the patient’s age. The physical examination reveals non-tender, fluctuating testicular swelling bilaterally with positive translucency. The swelling decreases slightly in the supine position and there is a positive cough impulse sign. A sonographic image is shown below. Which of the following statements about the patient’s condition is correct?
A 9-year-old boy is brought to the office due to exertional dyspnea and fatigability. He tires easily when walking or playing. His parents say that he was diagnosed with a congenital heart disease during his infancy, but they refused any treatment. They do not remember much about his diagnosis. The patient also had occasional respiratory infections throughout childhood that did not require hospitalization. He takes no medications. The patient has no family history of heart disease. His vital signs iclude: heart rate 98/min, respiratory rate 16/min, temperature 37.2°C (98.9°F), and blood pressure of 110/80 mm Hg. Physical examination shows toe cyanosis and clubbing but no finger abnormalities. Cardiac auscultation reveals a continuous machine-like murmur. All extremity pulses are full and equal. Which of the following is the most likely diagnosis?
A 3500-g (7.7-lbs) girl is delivered at 39 weeks' gestation to a 27-year-old woman, gravida 2, para 1. Apgar scores are 8 and 9 at 1 and 5 minutes, respectively. The mother had regular prenatal visits throughout the pregnancy. She did not smoke or drink alcohol. She took multivitamins as prescribed by her physician. The newborn appears active. The girl's temperature is 37°C (98.6°F), pulse is 120/min, and blood pressure is 55/35 mm Hg. Examination in the delivery room shows clitoromegaly. One day later, laboratory studies show: Hemoglobin 12.8 g/dL Leukocyte count 6,000/mm3 Platelet count 240,000/mm3 Serum Na+ 133 mEq/L K+ 5.2 mEq/L Cl− 101 mEq/L HCO3− 21 mEq/L Urea nitrogen 15 mg/dL Creatinine 0.8 mg/dL Ultrasound of the abdomen and pelvis shows normal uterus and normal ovaries. Which of the following is the most appropriate next step in the management of this newborn patient?
Practice by Chapter
Neural tube defects
Practice Questions
Congenital heart defects
Practice Questions
Gastrointestinal malformations
Practice Questions
Genitourinary anomalies
Practice Questions
Craniofacial anomalies
Practice Questions
Skeletal dysplasias
Practice Questions
Chromosomal disorders
Practice Questions
Teratogenic exposures
Practice Questions
Multiple malformation syndromes
Practice Questions
Prenatal diagnosis of congenital defects
Practice Questions
Surgical management timing
Practice Questions
Long-term outcomes and follow-up
Practice Questions
Preventive strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app