
Brain tumors in children — MCQs

A 13-year-old boy is brought to the physician because of a 4-month history of worsening dizziness, nausea, and feeling clumsy. An MRI of the brain shows a well-demarcated, 4-cm cystic mass in the posterior fossa. The patient undergoes complete surgical resection of the mass. Pathologic examination of the surgical specimen shows parallel bundles of cells with eosinophilic, corkscrew-like processes. Which of the following is the most likely diagnosis?
A previously healthy 10-year-old boy is brought to the emergency department for the evaluation of one episode of vomiting and severe headache since this morning. His mother says he also had difficulty getting dressed on his own. He has not had any trauma. The patient appears nervous. His temperature is 37°C (98.6°F), pulse is 100/min, and blood pressure is 185/125 mm Hg. He is confused and oriented only to person. Ophthalmic examination shows bilateral optic disc swelling. There is an abdominal bruit that is best heard at the right costovertebral angle. A complete blood count is within normal limits. Which of the following is most likely to confirm the diagnosis?
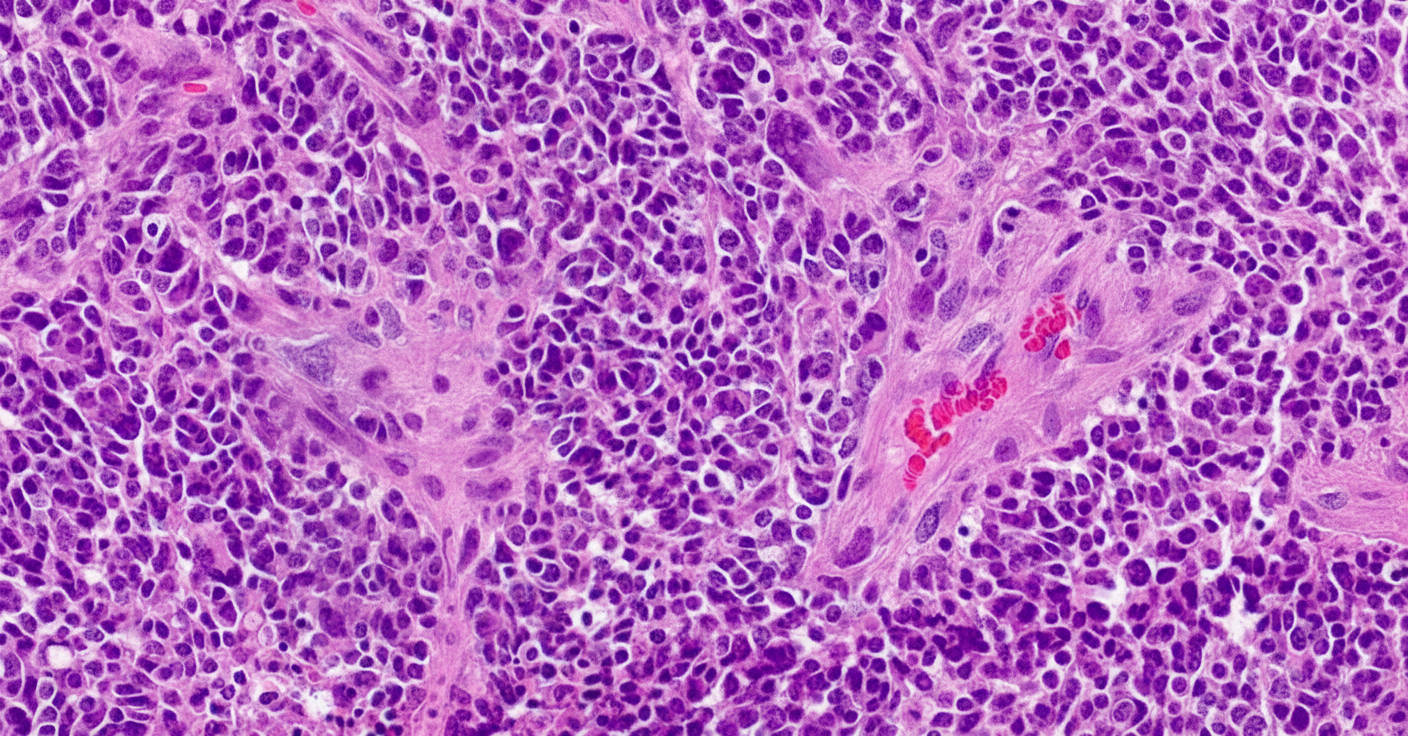
A previously healthy 4-year-old girl is brought to the physician for evaluation of a 3-week history of recurrent vomiting and difficulty walking. Examination shows a broad-based gait and bilateral optic disc swelling. An MRI shows an intracranial tumor. A ventriculoperitoneal shunt is placed, and surgical excision of the tumor is performed. A photomicrograph of a section of the tumor is shown. Which of the following is the most likely diagnosis?
A 10-year-old boy is brought to the emergency department by his parents because of a dull persistent headache beginning that morning. He has nausea and has vomited twice. During the past four days, the patient has had left-sided ear pain and fever, but his parents did not seek medical attention. He is from Thailand and is visiting his relatives in the United States for the summer. There is no personal or family history of serious illness. He is at the 45th percentile for height and 40th percentile for weight. He appears irritable. His temperature is 38.5°C (101.3°F), pulse is 110/min, and blood pressure is 98/58 mm Hg. The pupils are equal and reactive to light. Lateral gaze of the left eye is limited. The left tympanic membrane is erythematous with purulent discharge. There is no nuchal rigidity. Which of the following is the most appropriate next step in management?
A 7-year-old boy is brought to the physician because his parents are concerned about his early sexual development. He has no history of serious illness and takes no medications. His brother was diagnosed with testicular cancer 5 years ago and underwent a radical orchiectomy. The patient is at the 85th percentile for height and 70th percentile for weight. Examination shows greasy facial skin. There is coarse axillary hair. Pubic hair development is at Tanner stage 3 and testicular development is at Tanner stage 2. The remainder of the examination shows no abnormalities. An x-ray of the wrist shows a bone age of 10 years. Basal serum luteinizing hormone and follicle-stimulating hormone are elevated. An MRI of the brain shows no abnormalities. Which of the following is the most appropriate next step in management?
An 18-month-old boy is brought to the physician for a well-child examination. His mother is concerned because he is unable to walk on his own. He has been increasingly irritable over the past month, has been feeding poorly, and has had multiple episodes of vomiting. His immunizations are up-to-date. He is at the 50th percentile for height, 40th percentile for weight, and 98th percentile for head circumference. He appears lethargic. His vital signs are within normal limits. Examination shows a bulging anterior fontanelle. The child is unable to stand without support and falls if he attempts to walk. Muscle tone is increased and deep tendon reflexes are 4+ in the lower extremities. Examination of the back is unremarkable. An MRI of the brain shows symmetrical enlargement of all four ventricles. Which of the following is the most appropriate treatment in this patient?
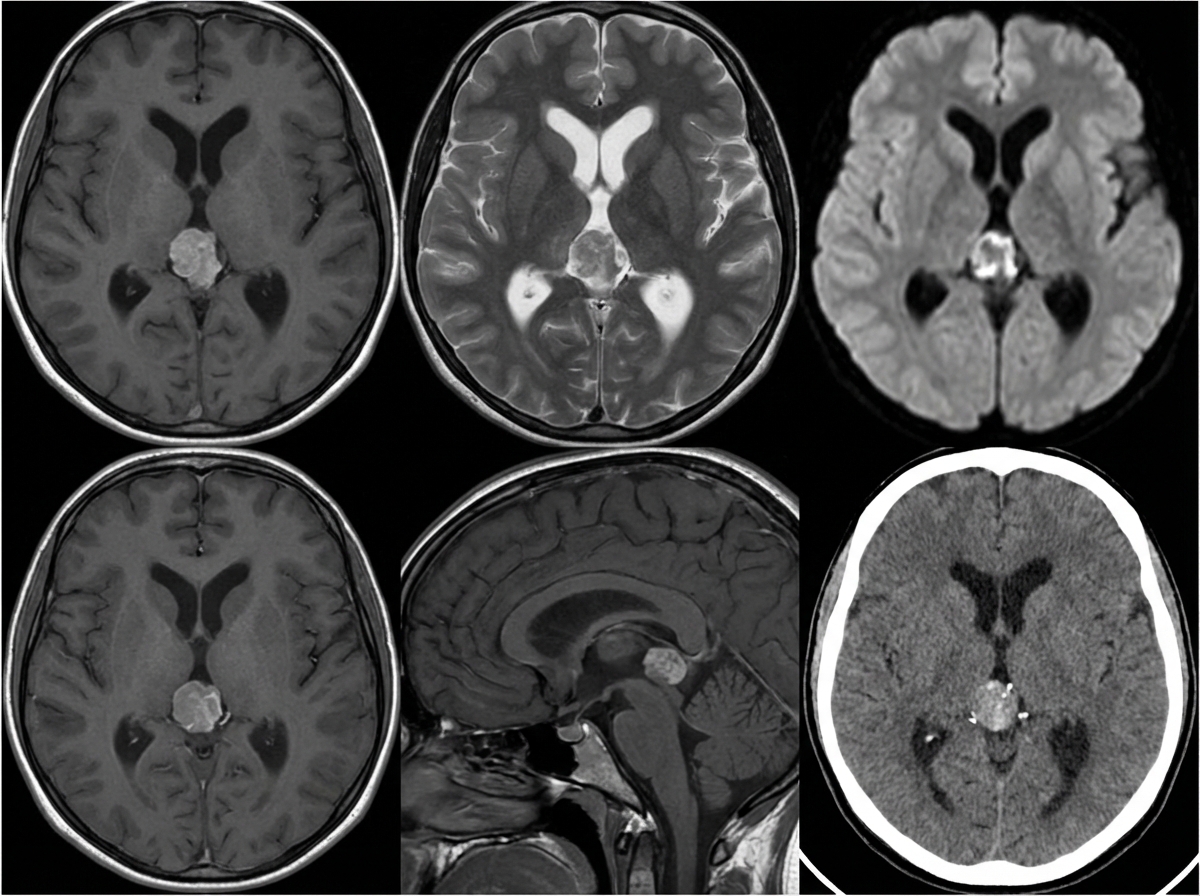
A 10-year-old girl is brought to the physician by her parents due to 2 months of a progressively worsening headache. The headaches were initially infrequent and her parents attributed them to stress from a recent move. However, over the last week the headaches have gotten significantly worse and she had one episode of vomiting this morning when she woke up. Her medical history is remarkable for a hospitalization during infancy for bacterial meningitis. On physical exam, the patient has difficulty looking up. The lower portion of her pupil is covered by the lower eyelid and there is sclera visible below the upper eyelid. A magnetic resonance imaging (MRI) of the brain is shown. Which of the following is the most likely diagnosis?
A 12-year-old boy is brought to the emergency department after he vomited and said he was having double vision in school. He also says that he has been experiencing morning headaches, nausea, and dizziness over the last month. He has no past medical history and is not taking any medications. Physical exam reveals a broad-based gait, dysmetria on finger-to-nose testing, and nystagmus. Both serum and urine toxicology are negative, and radiography reveals a solid mass in the midline cerebellum that enhances after contrast administration. Biopsy of this lesion reveals cells of primitive neuroectodermal origin. Which of the following would most likely be seen on histology of this lesion?
An inconsolable mother brings her 2-year-old son to the emergency room after finding a large amount of bright red blood in his diaper, an hour ago. She states that for the past week her son has been having crying fits while curling his legs towards his chest in a fetal position. His crying resolves either after vomiting or passing fecal material. Currently, the child is in no apparent distress. Physical examination with palpation in the gastric region demonstrates no acute findings. X-ray of the abdominal area demonstrates no acute findings. His current temperature is 36.5°C (97.8°F), heart rate is 93/min, blood pressure is 100/64 mm Hg, and respiratory rate is 26/min. His weight is 10.8 kg (24.0 lb), and height is 88.9 cm (35.0 in). Laboratory tests show the following: RBC count 5 million/mm3 Hematocrit 36% Hemoglobin 12 g/dL WBC count 6,000/mm3 Mean corpuscular volume 78 fL What is the most likely underlying embryological cause predisposing to this condition?
A 25-year-old man comes to the physician because of right-sided painless scrotal swelling that he noticed yesterday while taking a shower. He is currently sexually active with two female partners and uses condoms inconsistently. He immigrated to the US from Argentina 2 years ago. His immunization records are unavailable. He has smoked one pack of cigarettes daily for the last 5 years. He is 170 cm (5 ft 7 in) tall and weighs 70 kg (154 lb); BMI is 24.2 kg/m2. He appears healthy and well nourished. His temperature is 37°C (98.6°F), pulse is 72/min, and blood pressure is 125/75 mm Hg. The lungs are clear to auscultation. Cardiac examination shows no abnormalities. The abdomen is soft with dull lower abdominal discomfort. Testicular examination shows a solid mass in the right testis that is firm and nontender. A light held behind the scrotum does not shine through. The mass is not reduced when the patient is in a supine position. The remainder of the physical examination shows no abnormalities. Which of the following is the most likely diagnosis in this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app