
Medical Ethics — MCQs

On this page
A 81-year-old man presents to his cardiologist for ongoing management of mild heart failure. He has not had any changes in his cardiac function status and says that he is tolerating lisinopril without any major side effects. During the course of the visit, the patient says that he is unhappy with his urologist because he has been experiencing episodes of dizziness after starting prazosin for benign prostatic hyperplasia. He says that he feels these episodes were caused by malpractice on his urologist's behalf and is considering a lawsuit against his urologist. Which of the following is the most appropriate course of action for the cardiologist?
A 65-year-old non-smoking woman with no symptoms comes to your clinic to establish care with a primary care provider. She hasn’t seen a doctor in 12 years and states that she feels very healthy. You realize that guidelines by the national cancer organization suggest that she is due for some cancer screening tests, including a mammogram for breast cancer, a colonoscopy for colon cancer, and a pap smear for cervical cancer. These three screening tests are most likely to be considered which of the following?
Two hours after admission to the intensive care unit, a 56-year-old man with necrotizing pancreatitis develops profound hypotension. His blood pressure is 80/50 mm Hg and he is started on vasopressors. A central venous access line is placed. Which of the following is most likely to decrease the risk of complications from this procedure?
A 34-year-old primigravida was brought to an obstetric clinic with a chief complaint of painless vaginal bleeding. She was diagnosed with placenta praevia and transfused with 2 units of whole blood. Five hours after the transfusion, she developed a fever and chills. How could the current situation be prevented?
A 35-year-old woman with no significant past medical history is brought in by ambulance after a major motor vehicle collision. Temperature is 97.8 deg F (36.5 deg C), blood pressure is 76/40, pulse is 110/min, and respirations are 12/min. She arouses to painful stimuli and makes incomprehensible sounds, but is unable to answer questions. Her abdomen is distended and diffusely tender to palpation. Bedside ultrasound shows blood in the peritoneal cavity. Her husband rushes to the bedside and states she is a Jehovah’s Witness and will refuse blood products. No documentation of blood refusal is available for the patient. What is the most appropriate next step in management?
A 72-year-old woman is brought to the emergency department with dyspnea for 2 days. She is on regular hemodialysis at 3 sessions a week but missed her last session due to an unexpected trip. She has a history of congestive heart failure. After urgent hemodialysis, the patient’s dyspnea does not improve as expected. The cardiologist is consulted. After evaluation of the patient, he notes in the patient’s electronic record: “the patient does not have a chronic heart condition and a cardiac cause of dyspnea is unlikely.” The following morning, the nurse finds the cardiologist’s notes about the patient not having congestive heart failure odd. The patient had a clear history of congestive heart failure with an ejection fraction of 35%. After further investigation, the nurse realizes that the cardiologist evaluated the patient’s roommate. She is an elderly woman with a similar first name. She is also on chronic hemodialysis. To prevent similar future errors, the most appropriate strategy is to use which of the following?
A 25-year-old man is admitted to the emergency department because of an episode of acute psychosis with suicidal ideation. He has no history of serious illness and currently takes no medications. Despite appropriate safety precautions, he manages to leave the examination room unattended. Shortly afterward, he is found lying outside the emergency department. A visitor reports that she saw the patient climbing up the facade of the hospital building. He does not respond to questions but points to his head when asked about pain. His pulse is 131/min, respirations are 22/min, and blood pressure is 95/61 mm Hg. Physical examination shows a 1-cm head laceration and an open fracture of the right tibia. He opens his eyes spontaneously. Pupils are equal, round, and reactive to light. Breath sounds are decreased over the right lung field, and the upper right hemithorax is hyperresonant to percussion. Which of the following is the most appropriate next step in management?
A 17-year-old girl makes an appointment with her pediatrician because she is concerned that she may have gotten a sexually transmitted infection. Specifically, she had unprotected sex two weeks ago and has since been experiencing painful urination and abdominal pain. Laboratory tests confirm a diagnosis of Chlamydial infection. At this point, the girl says that she wants to personally give permission to be treated rather than seek consent from her parents because they do not know that she is in a relationship. She also asks that the diagnosis not be reported to anyone. What should the physician do with regards to these two patient requests?
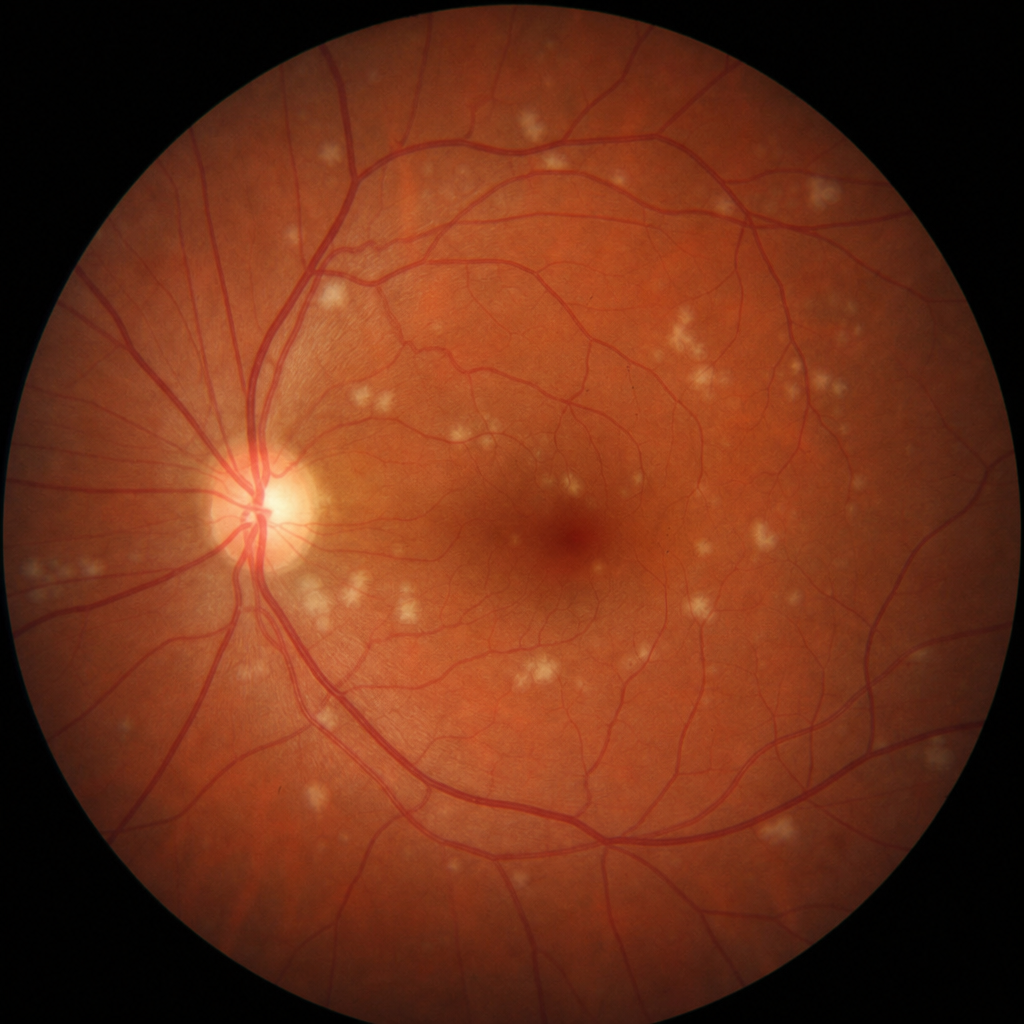
A 3-year-old male is brought to the emergency department by his parents, who report he fell off the couch. On physical examination and imaging, the child shows evidence of multiple healed fractures in various stages of healing and unexplained bruising over his trunk and extremities inconsistent with the reported mechanism of injury. On eye exam, the child's sclerae appear blue, and results of a fundoscopic exam are shown in Image A. What is the most appropriate next step in the care of this patient?
A 14-year-old girl presents to the emergency room complaining of abdominal pain. She was watching a movie 3 hours prior to presentation when she developed severe non-radiating right lower quadrant pain. The pain has worsened since it started. She also had non-bloody non-bilious emesis 1 hour ago and continues to feel nauseated. Her temperature is 101°F (38.3°C), blood pressure is 130/90 mmHg, pulse is 110/min, and respirations are 22/min. On exam, she has rebound tenderness at McBurney point and a positive Rovsing sign. She is stabilized with intravenous fluids and pain medication and is taken to the operating room to undergo a laparoscopic appendectomy. While in the operating room, the circulating nurse leads the surgical team in a time out to ensure that introductions are made, the patient’s name and date of birth are correct, antibiotics have been given, and the surgical site is marked appropriately. This process is an example of which of the following human factor engineering elements?
Practice by Chapter
Ethical principles (autonomy, beneficence, non-maleficence, justice)
Practice Questions
Ethical frameworks for decision-making
Practice Questions
Ethics committees and consultations
Practice Questions
Conflicts of interest
Practice Questions
Truth-telling and disclosure
Practice Questions
Confidentiality boundaries
Practice Questions
Resource allocation ethics
Practice Questions
Research ethics and IRBs
Practice Questions
Reproductive ethics
Practice Questions
Genetic testing ethics
Practice Questions
Professional boundaries
Practice Questions
Medical error disclosure
Practice Questions
Ethics of emerging technologies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app