
Renal vascular diseases — MCQs

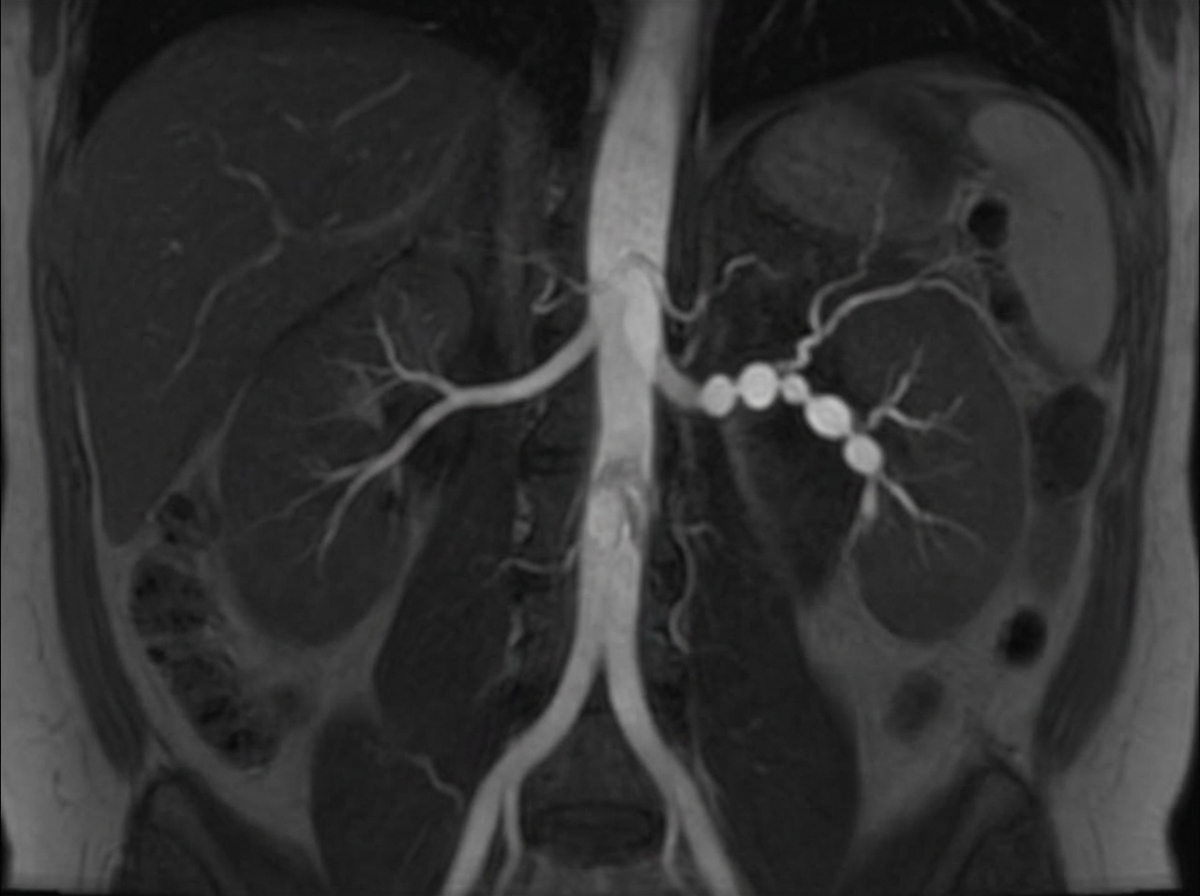
A 31-year-old woman returns to her primary care provider for a follow-up visit. At a routine health maintenance visit 2 months ago, her blood pressure (BP) was 181/97 mm Hg. She has adhered to a low-salt diet and exercises regularly. On repeat examination 1 month later, her BP was 178/93, and she was prescribed hydrochlorothiazide and lisinopril. The patient denies any complaint, except for occasional headaches. Now, her BP is 179/95 in the right arm and 181/93 in the left arm. Physical examination reveals an abdominal bruit that lateralizes to the left. A magnetic resonance angiogram of the renal arteries is shown in the image. Which of the following is the best next step for the management of this patient condition?
A 60-year-old African American woman presents to her family physician with shortness of breath on exertion. She also describes shortness of breath when she lies down to go to bed at night, as well as recent swelling in her ankles. Past medical history is significant for long-standing hypertension, for which she takes amlodipine and lisinopril. Her temperature is 36.8°C (98.2°F), the heart rate is 90/min, the respiratory rate is 15/min, and the blood pressure is 135/80 mm Hg. The physical exam is significant for JVD, lower extremity pitting edema, laterally displaced PMI, left ventricular heave, bilateral pulmonary crackles, and an S4 heart sound. Chest X-ray demonstrates pulmonary vascular congestion, Kerley B lines, and cardiomegaly. Echocardiogram demonstrates a preserved ejection fraction. Kidney biopsy would likely demonstrate which of the following?
A 50-year-old man is brought to the hospital after being found unresponsive in his bed in the morning. He is declared dead on arrival in the emergency room. His wife states that he always had uncontrolled hypertension despite being on multiple medications. An autopsy is performed, and the cause of his death is found to be a hemorrhage in his right basal ganglia. On microscopic examination, the branches of the renal artery have concentric endothelial proliferation with prominent narrowing of the lumen resulting in focal ischemia and hemorrhage of the renal parenchyma. Which of the following is most likely related to the findings in this patient?
A previously healthy 40-year-old woman comes to the physician because of a 3-day history of fever, headaches, and fatigue. She also reports a persistent tingling sensation in her right hand and numbness in her right arm that started this morning. Physical examination shows pallor, mild scleral icterus, and petechiae on her forearms and legs. On mental status examination, she appears confused and is only oriented to person. Laboratory studies show: Hemoglobin 11.1 g/dL Platelet count 39,500/mm3 Bleeding time 9 minutes Prothrombin time 14 seconds Partial thromboplastin time 35 seconds Serum Creatinine 1.7 mg/dL Total bilirubin 2.1 mg/dL A peripheral blood smear shows fragmented erythrocytes. Which of the following is the most likely underlying cause of this patient's condition?
A 53-year-old woman presents with a severe headache, nausea, and vomiting for the past 48 hours. Vitals show a blood pressure of 220/134 mm Hg and a pulse of 88/min. Urinalysis shows a 2+ proteinuria and RBC casts. Which of the following renal lesions is most likely to be seen in this patient?
A 62-year-old man comes to the physician because of fatigue and swelling of the lower legs for 3 weeks. One year ago, he had an 85% stenosis in the left anterior descending artery, for which he received 2 stents. He was diagnosed with hepatitis C 5 years ago. He has type 2 diabetes mellitus and arterial hypertension. Current medications include aspirin, metformin, and ramipril. He does not smoke or drink alcohol. His temperature is 37°C (98.6°F), pulse is 92/min, and blood pressure is 142/95 mm Hg. Examination shows 2+ pretibial edema bilaterally. The remainder of the examination shows no abnormalities. Laboratory studies show: Hemoglobin 10.2 g/dL Leukocyte count 6500/mm3 Platelet count 188,000/mm3 Serum Na+ 137 mEq/L Cl− 105 mEq/L K+ 5.2 mEq/L Urea nitrogen 60 mg/dL Glucose 110 mg/dL Creatinine 3.9 mg/dL Albumin 3.6 g/dL HbA1C 6.8% Urine Blood negative Glucose 1+ Protein 3+ WBC 0–1/hpf A renal biopsy shows sclerosis in the capillary tufts and arterial hyalinosis. Which of the following is the most likely underlying mechanism of this patient's findings?
A 48-year-old man is brought to the emergency department by his wife because of a 3-day history of increasing confusion and lethargy. He complains of decreased urine output and abdominal pain for the past month. Two months ago, he was hospitalized for pyelonephritis and treated with ceftriaxone. He has a history of chronic hepatitis C. He does not take any medications. He appears pale and irritable. His temperature is 37°C (98.6°F), pulse is 90/min, and blood pressure is 98/60 mm Hg. On mental status examination, he is oriented to person but not to time or place. Physical examination shows scleral icterus and jaundice. There is 2+ pitting edema of the lower extremities. The abdomen is distended with a positive fluid wave. Laboratory studies show: Hemoglobin 10.1 g/dL Leukocyte count 4300/mm3 Platelet count 89,000/mm3 Prothrombin time 19 sec Serum Urea nitrogen 71 mg/dL Glucose 99 mg/dL Creatinine 3.5 mg/dL ALT 137 mg/dL AST 154 mg/dL Urinalysis shows no abnormalities. The FeNa is < 1%. Ultrasound of the kidneys is unremarkable. Intravenous fluids are administered for 36 hours but do not improve urine output. Which of the following is the most likely cause of the kidney dysfunction in this patient?
A 60-year-old male presents for a routine health check-up. The patient complains of reduced exercise tolerance for the past 2 years. Also, in the past year, he has noticed chest pain after climbing the stairs in his home. He has no significant past medical history or current medications. The patient reports a 45-pack-year smoking history. The vital signs include temperature 37.0°C (98.6°F), blood pressure 160/100 mm Hg, pulse 72/min, respiratory rate 15/min, and oxygen saturation 99% on room air. His body mass index (BMI) is 34 kg/m2. Physical examination is unremarkable. Laboratory studies show: Serum total cholesterol 265 mg/dL HDL 22 mg/dL LDL 130 mg/dL Triglycerides 175 mg/dL HDL: high-density lipoprotein; LDL: low-density lipoprotein Which of the following vascular pathologies is most likely present in this patient?
A 67-year-old man presents with pain in both legs. He says the pain is intermittent in nature and has been present for approximately 6 months. The pain increases with walking, especially downhill, and prolonged standing. It is relieved by lying down and leaning forward. Past medical history is significant for type 2 diabetes mellitus, hypercholesterolemia, and osteoarthritis. The patient reports a 56-pack-year history but denies any alcohol or recreational drug use. His vital signs include: blood pressure 142/88 mm Hg, pulse 88/min, respiratory rate 14/min, temperature 37°C (98.6°F). On physical examination, the patient is alert and oriented. Muscle strength is 5/5 in his upper and lower extremities bilaterally. Babinski and Romberg tests are negative. Pulses measure 2+ in upper and lower extremities bilaterally. Which of the following is the next best step in the management of this patient?
A 70-year-old man is brought to the emergency department by his wife because of lethargy, confusion, and nausea for the past 2 days. He has previously been healthy and has no past medical history. His only medications are a daily multivitamin and acetaminophen, which he takes daily for hip pain. Vital signs are within normal limits. He is disoriented to place and time but recognizes his wife. The remainder of his physical examination shows no abnormalities. Laboratory studies show a hemoglobin concentration of 9.1 g/dL, a serum calcium concentration of 14.7 mg/dL, and a serum creatinine of 2.2 mg/dL (previously 0.9 mg/dL). Which of the following is the most likely underlying mechanism of this patient's condition?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app