
Renal pathology — MCQs

On this page
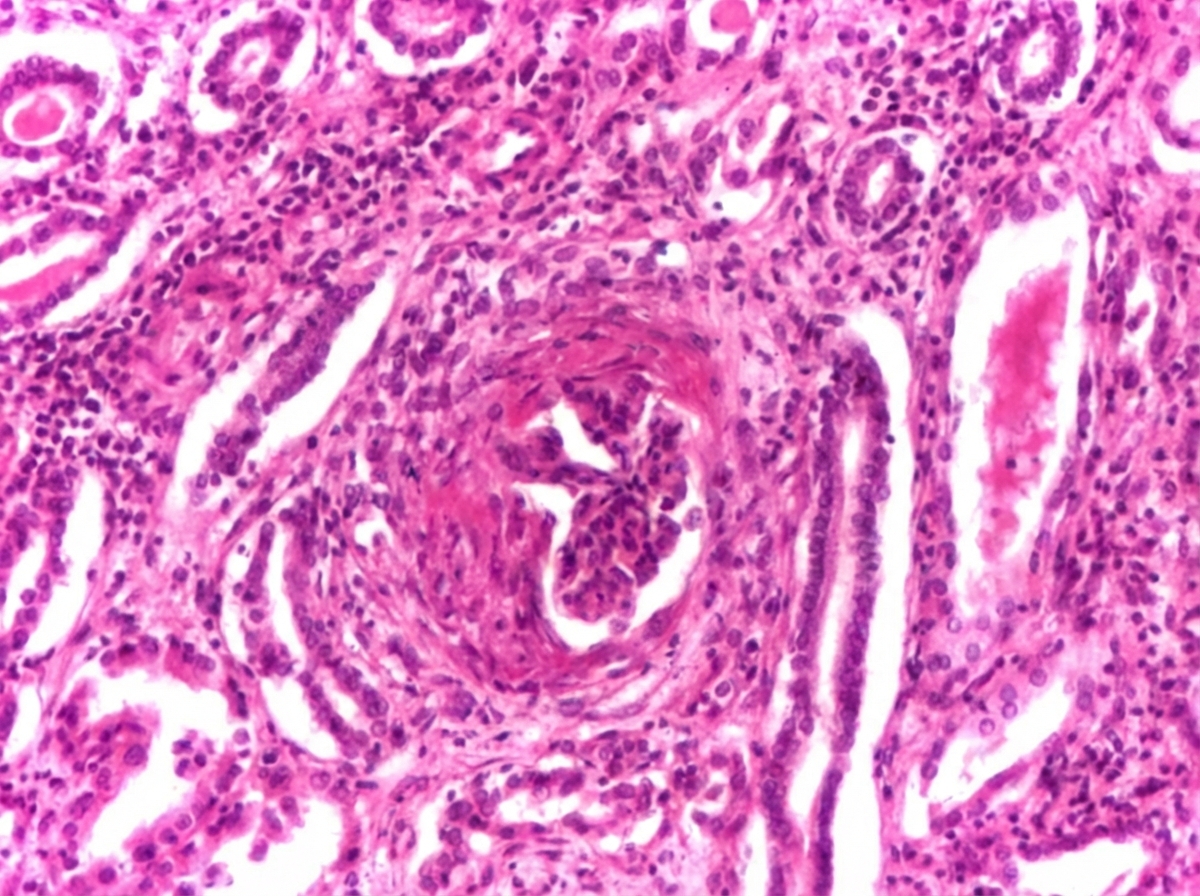
Kidney biopsy report shown in the image depicts:
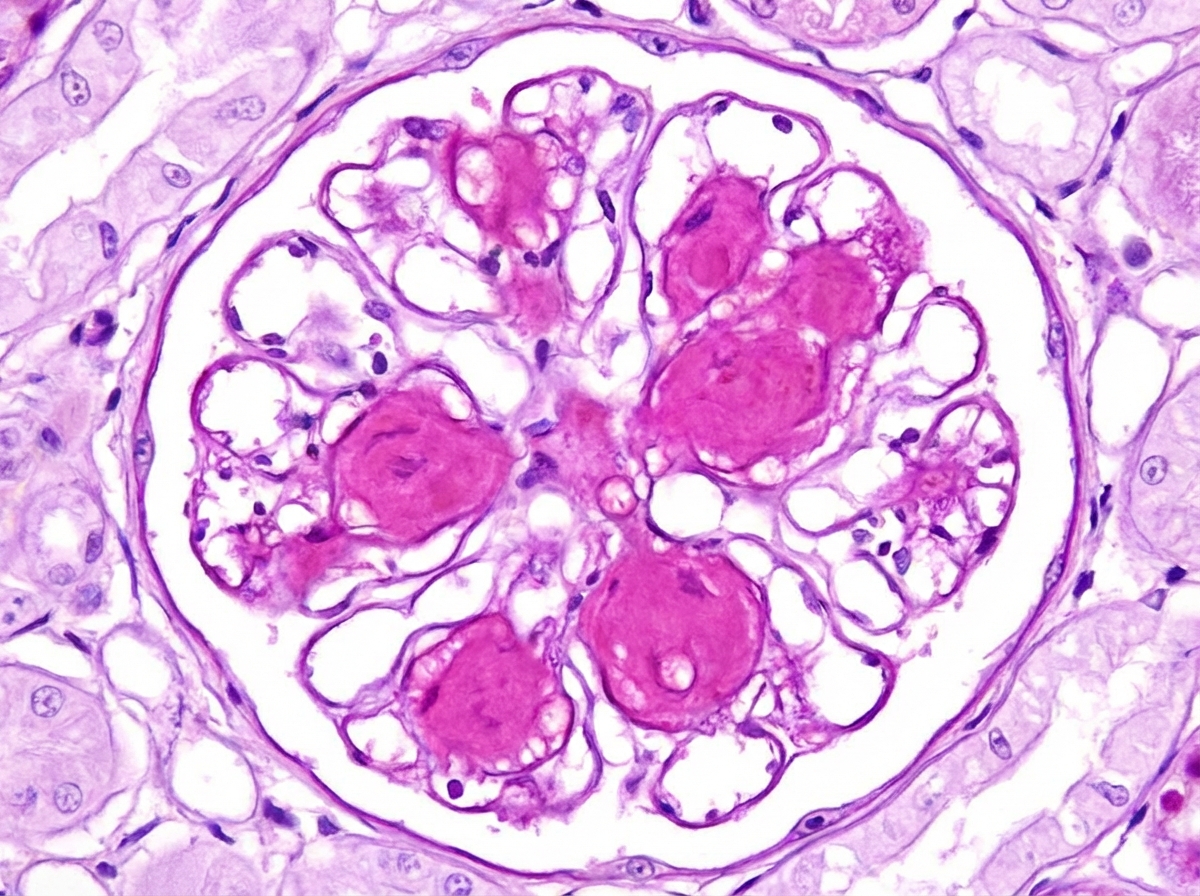
Comment on the diagnosis of light microscopy finding in kidney biopsy. (Recent NEET Pattern 2016-17)
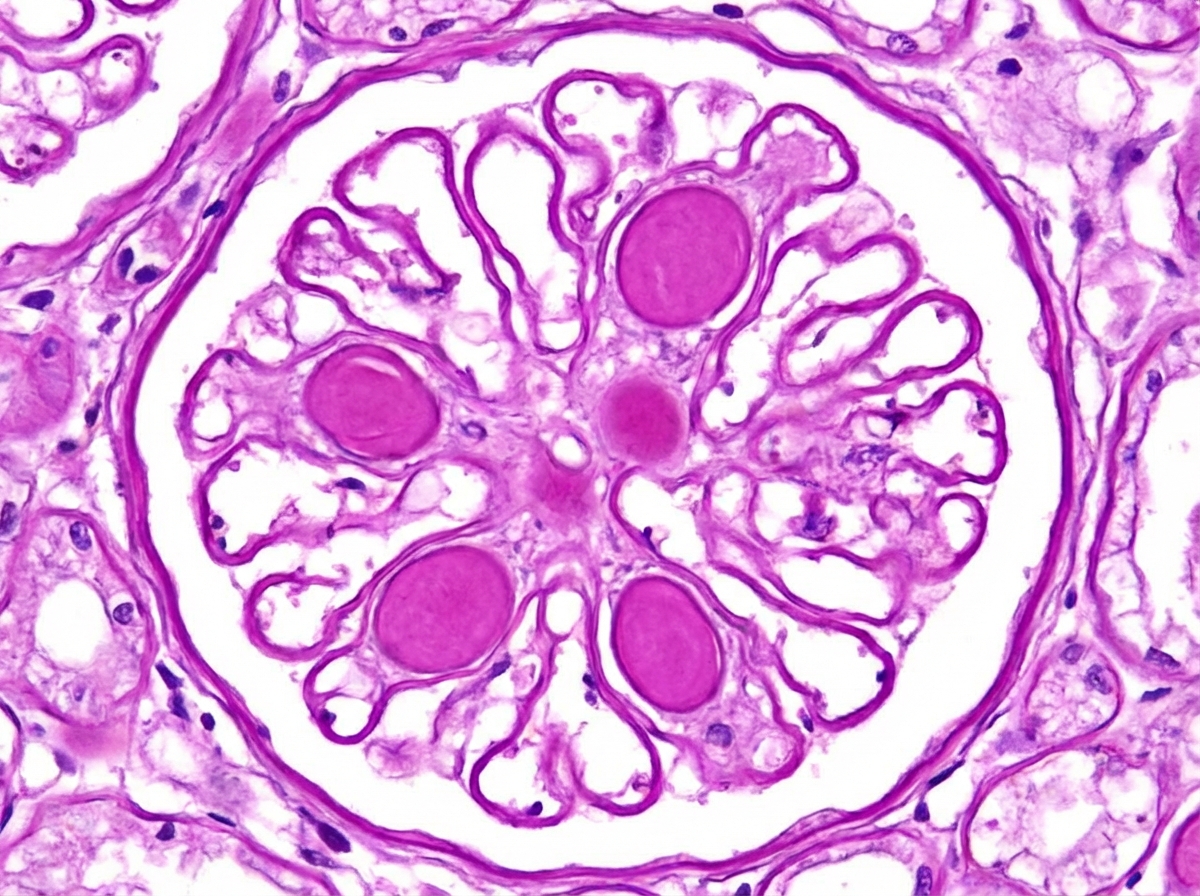
All are true about the presentation in kidney biopsy shown except: (Recent NEET Pattern 2016-17)
All are causes of this glomerular presentation except: (Recent NEET Pattern 2016-17)
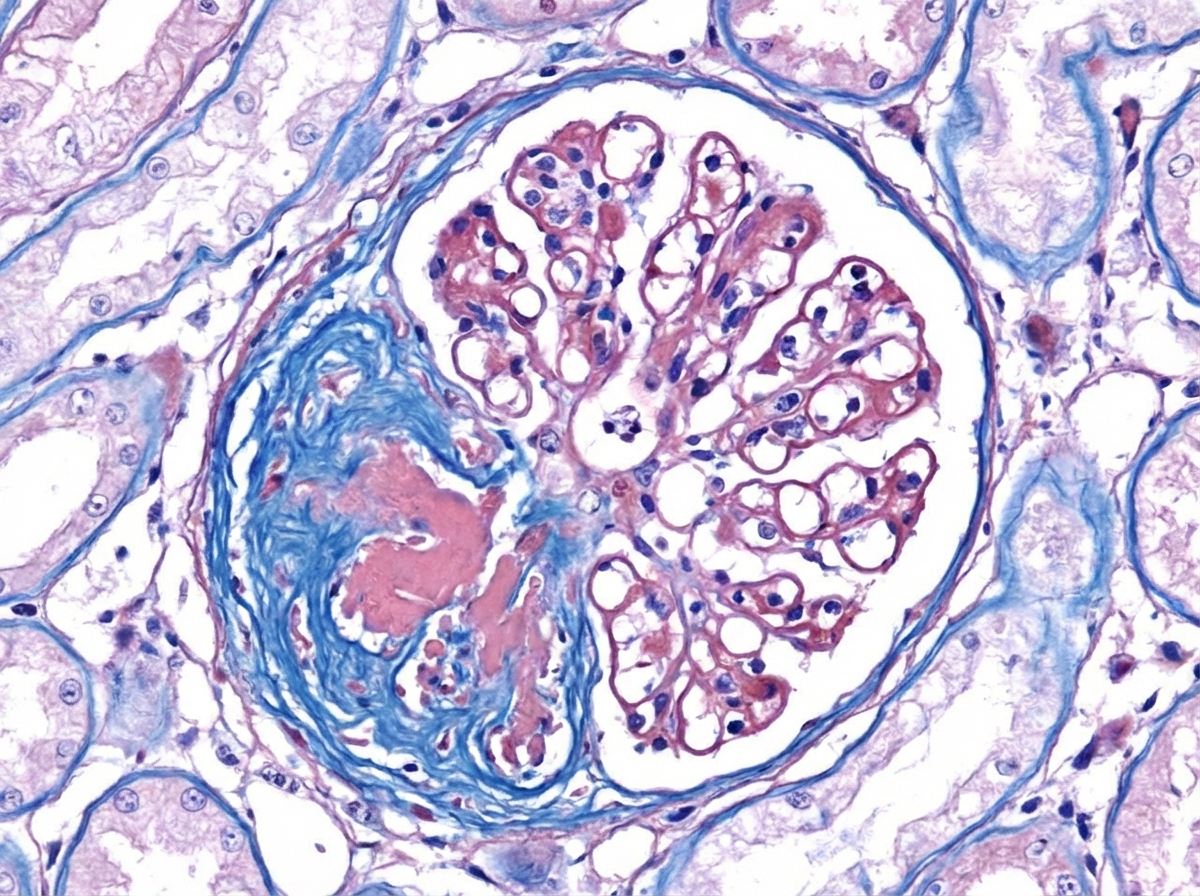
Comment on the vascular change present in the kidney biopsy slide. (Recent NEET Pattern 2016-17)
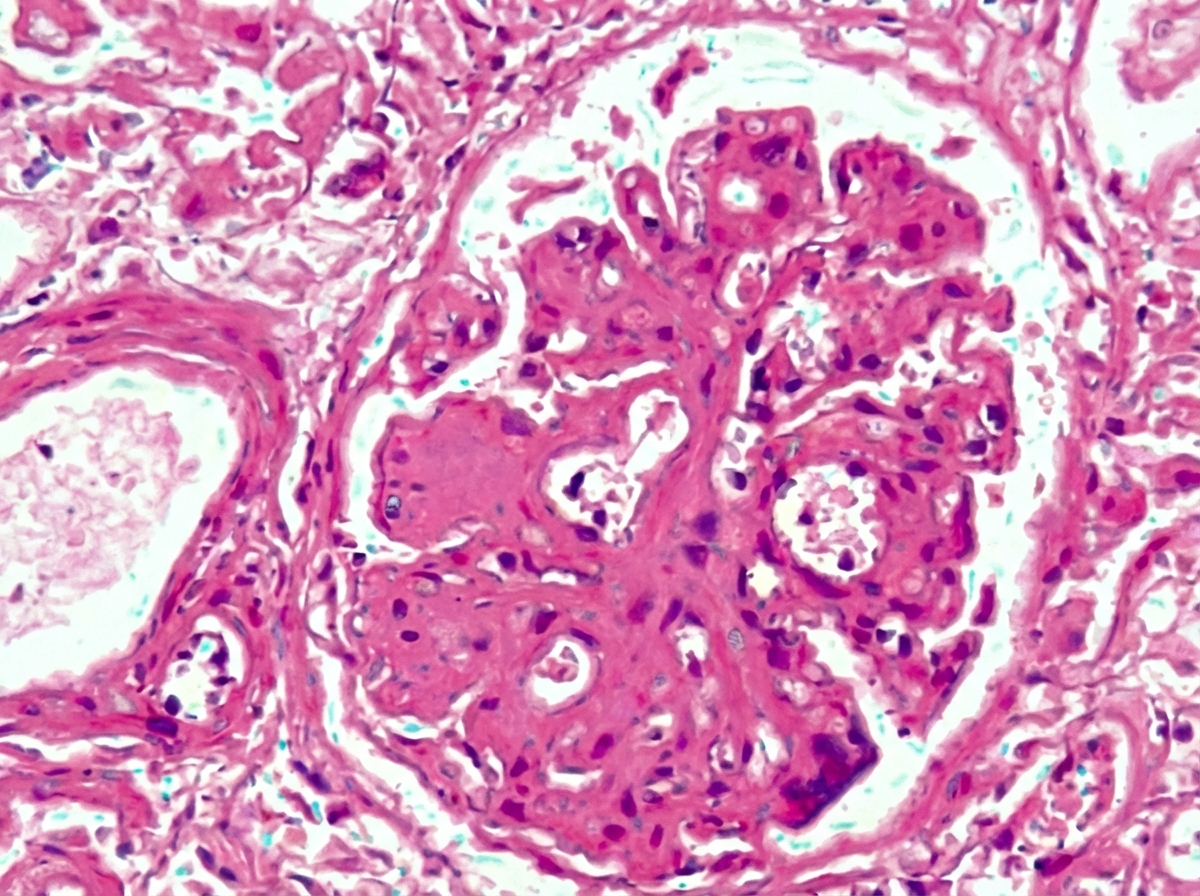
The image shows:
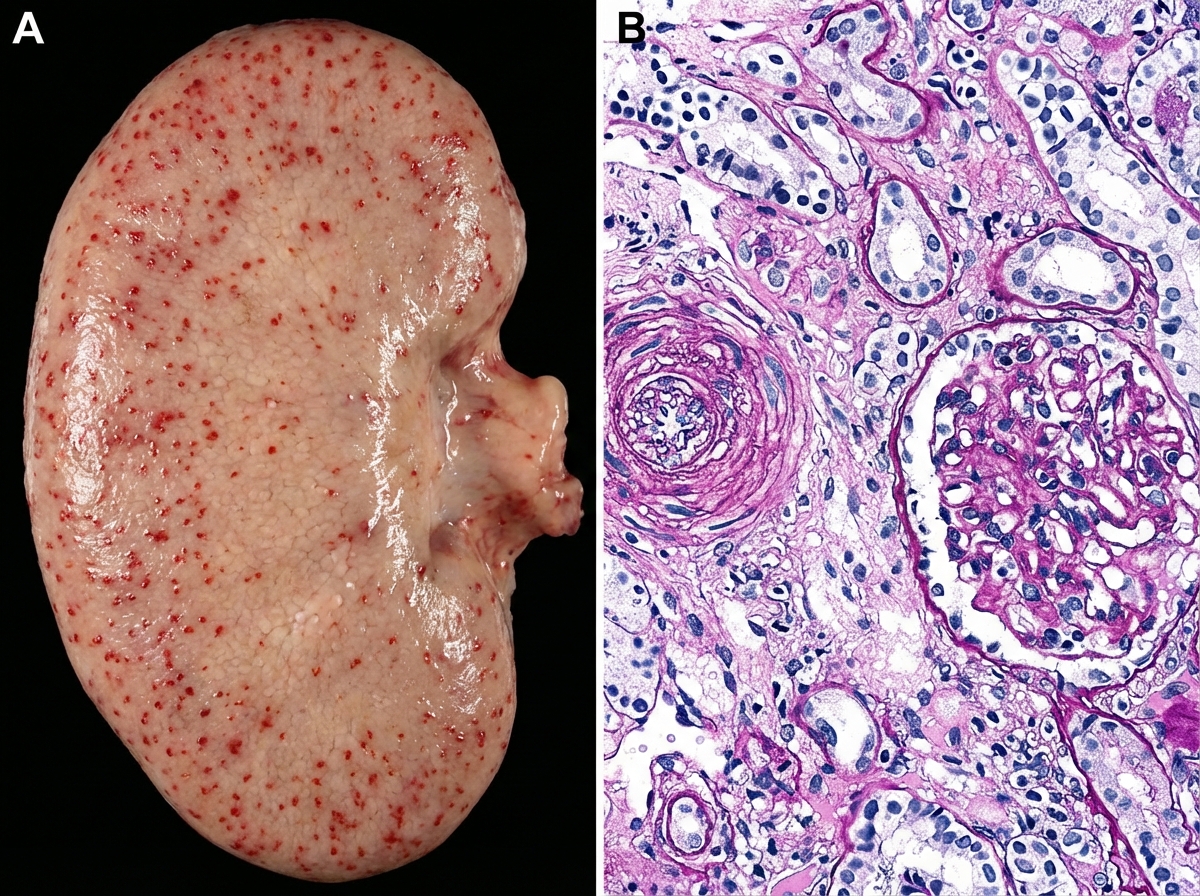
Kidney specimen of 40 -year-old man is shown below. All are true about the condition shown in the figure except:

The image shows presence of:
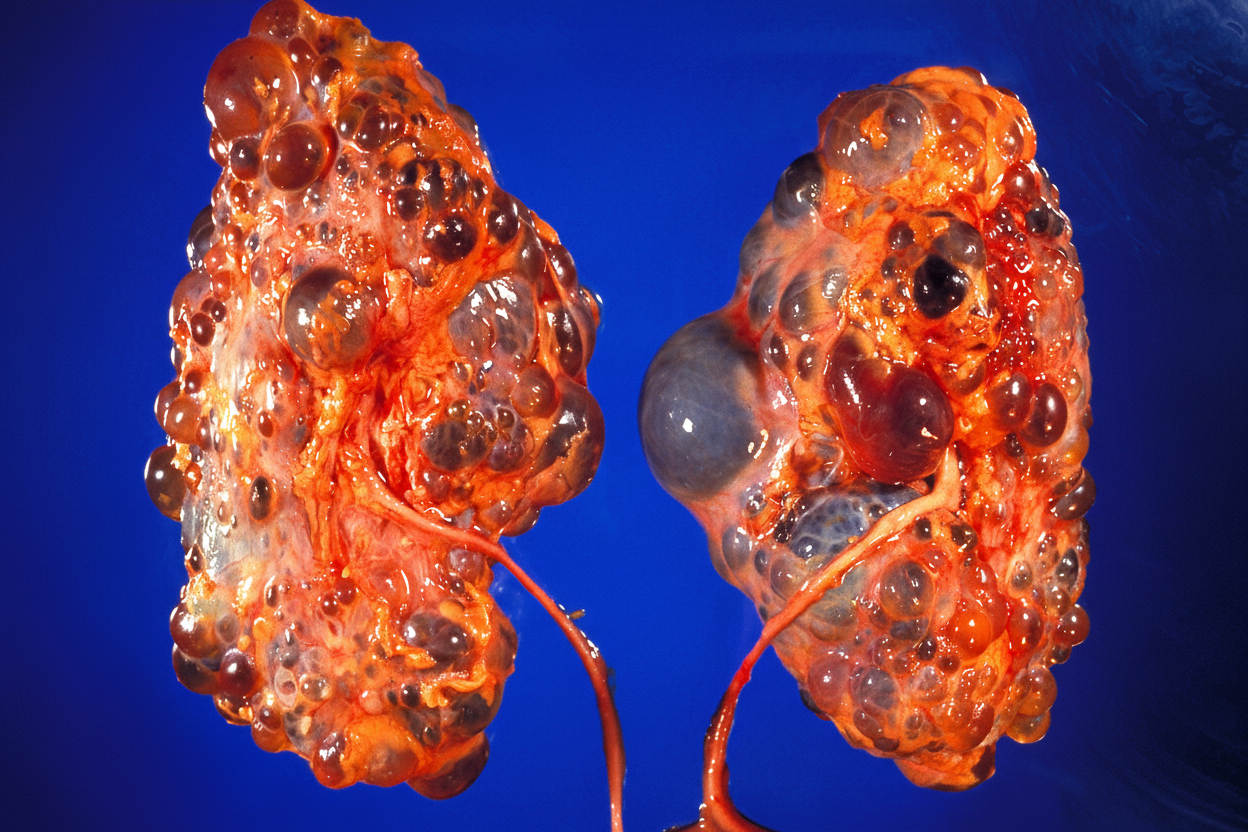
The kidneys shown in this image are from a 24-year-old man who was found unresponsive and died shortly after complaining of a sudden severe headache. What would have been the most likely cause of his death?

A 28-year-old female with a history of recurrent urinary tract infections caused by a urease-positive organism presents with flank pain. Urine pH is found to be alkaline. On surgical extraction of the kidney, patient's presentation is similar to that given in the image. What is the likely diagnosis?

Practice by Chapter
Congenital renal anomalies
Practice Questions
Glomerular diseases overview
Practice Questions
Nephritic syndrome disorders
Practice Questions
Nephrotic syndrome disorders
Practice Questions
Rapidly progressive glomerulonephritis
Practice Questions
Tubulointerstitial diseases
Practice Questions
Acute tubular necrosis
Practice Questions
Renal vascular diseases
Practice Questions
Pyelonephritis and urinary tract infections
Practice Questions
Renal cystic diseases
Practice Questions
Obstructive uropathies
Practice Questions
Renal tumors
Practice Questions
Kidney transplant pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app