
Renal pathology — MCQs

On this page
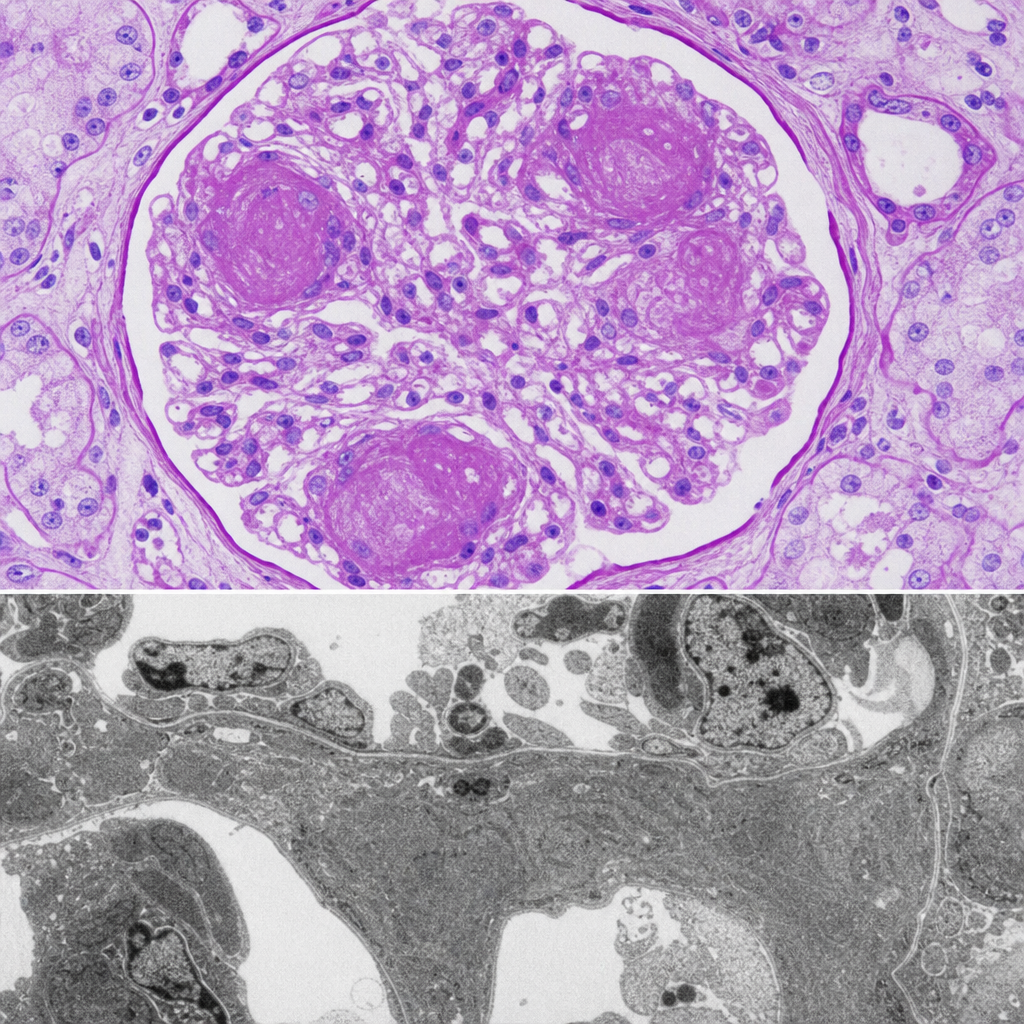
A 45-year-old woman with longstanding type 2 diabetes mellitus and hypertension presents with nephrotic-range proteinuria. Renal biopsy is performed. The photomicrograph shows PAS-positive, ovoid to spherical, acellular deposits within the mesangium of glomeruli, expanding the mesangial matrix and compressing adjacent capillary loops. Electron microscopy confirms mesangial matrix expansion without electron-dense subepithelial or subendothelial deposits. Which of the following named lesions is depicted?
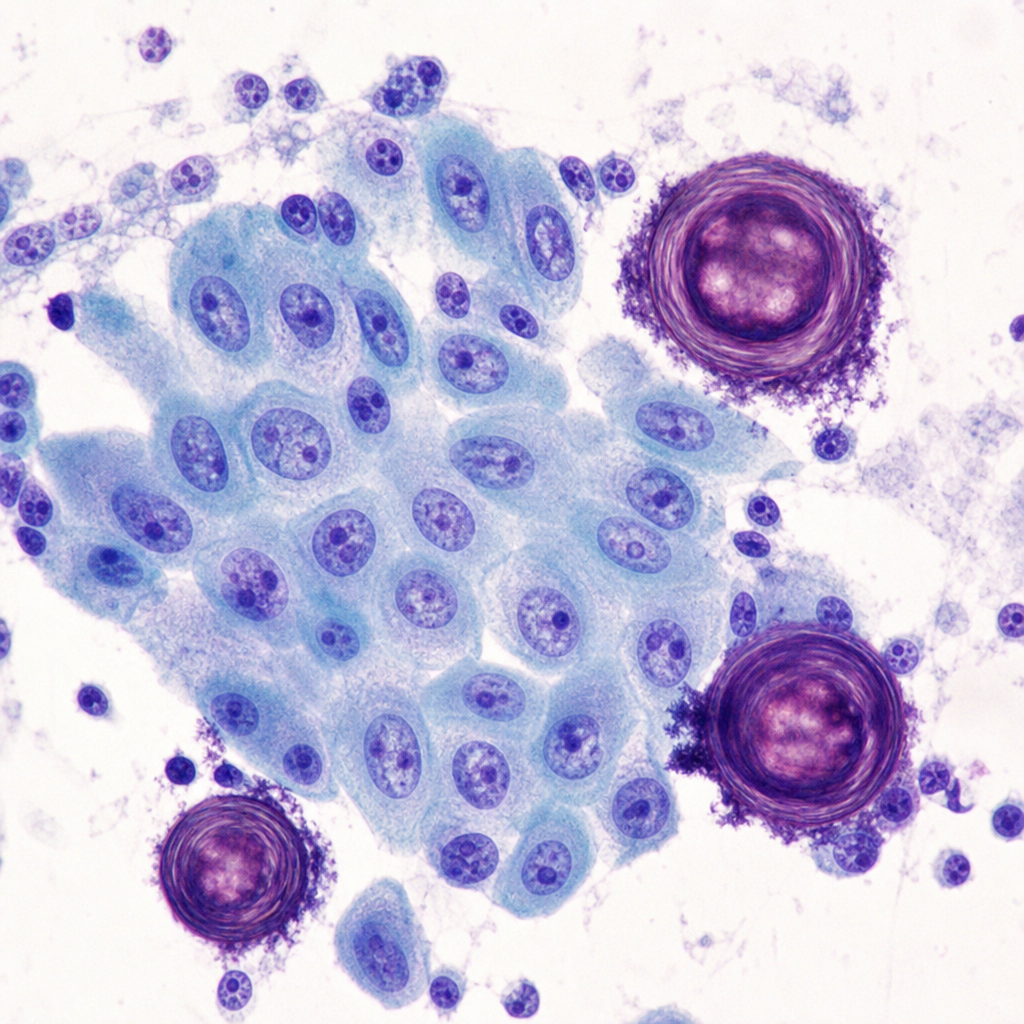
A 34-year-old woman is found to have a 2.8 cm solitary thyroid nodule on ultrasound. Fine-needle aspiration cytology is performed. The photomicrograph demonstrates follicular cells arranged in overlapping clusters with enlarged nuclei showing longitudinal grooves, pale 'ground-glass' chromatin, and intranuclear cytoplasmic pseudoinclusions. Scattered among the follicular cells are concentrically laminated calcified spherical structures. Which of the following mechanisms best explains the formation of the calcified structures seen in this specimen?
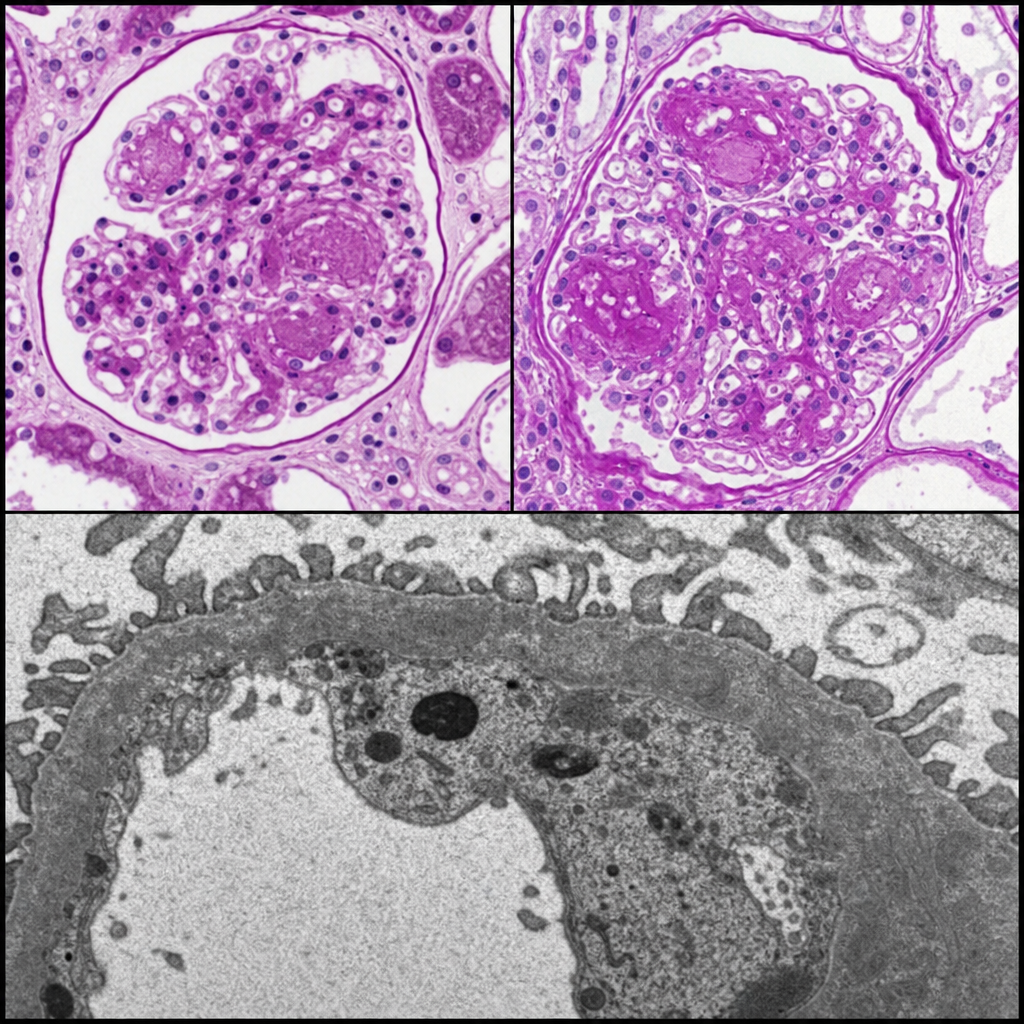
A 62-year-old man with poorly controlled type 2 diabetes mellitus for 22 years presents with proteinuria of 4.2 g/day and a creatinine of 2.8 mg/dL. A renal biopsy is performed. Light microscopy reveals nodular deposits of eosinophilic material within the mesangium of glomeruli, with peripheral capillary loop compression. PAS stain shows the nodules to be strongly positive. Electron microscopy demonstrates increased mesangial matrix and basement membrane thickening without electron-dense deposits. Which of the following best describes the pathological process responsible for the nodular mesangial deposits seen in this biopsy?
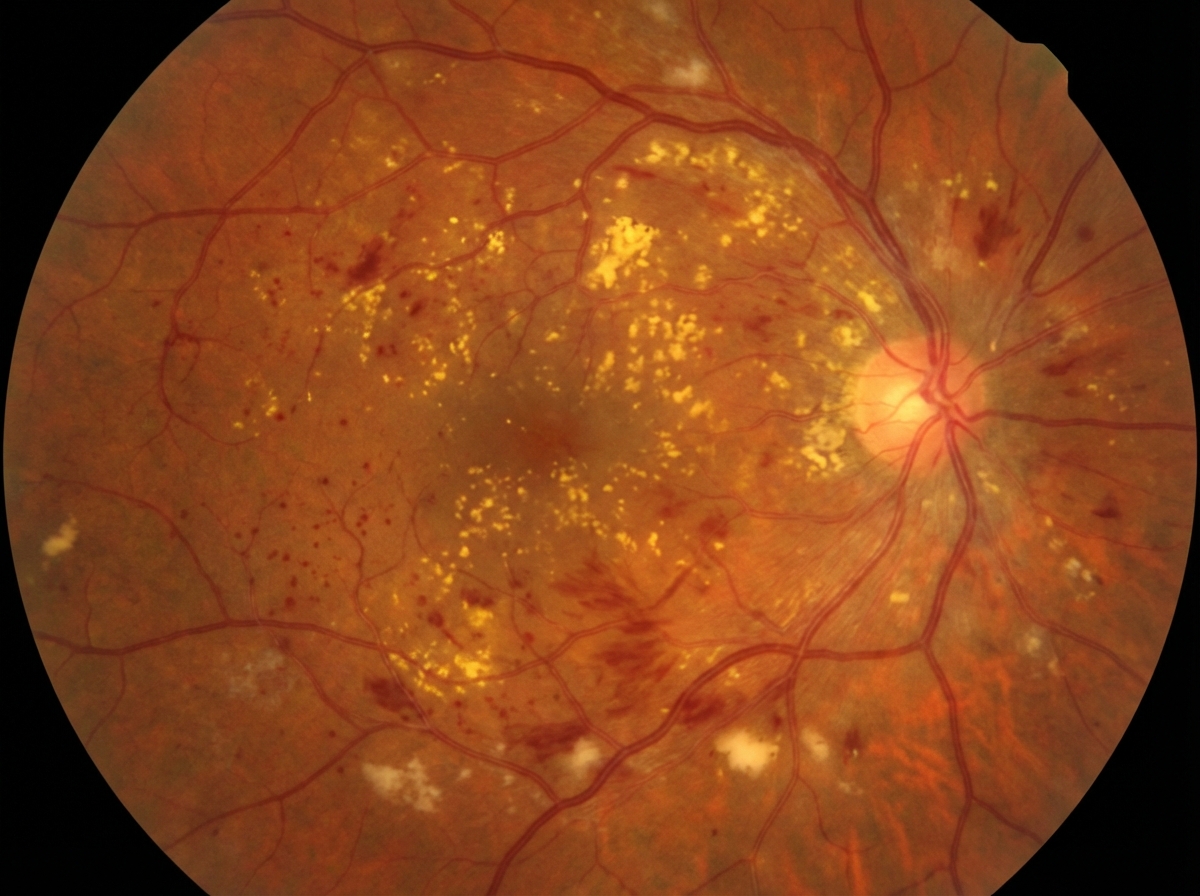
A 58-year-old woman with HbA1c of 10 % is referred to an ophthalmologist because of vision loss. An image of her retina is shown below, If this patient were to undergo renal biopsy, what will be the pathologic findings?
All are true about the condition shown except:
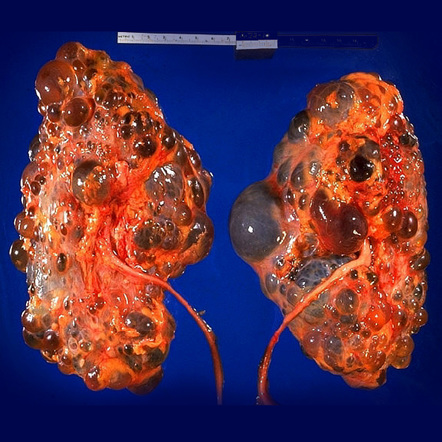
Which is not a true statement about this anomaly of kidney?

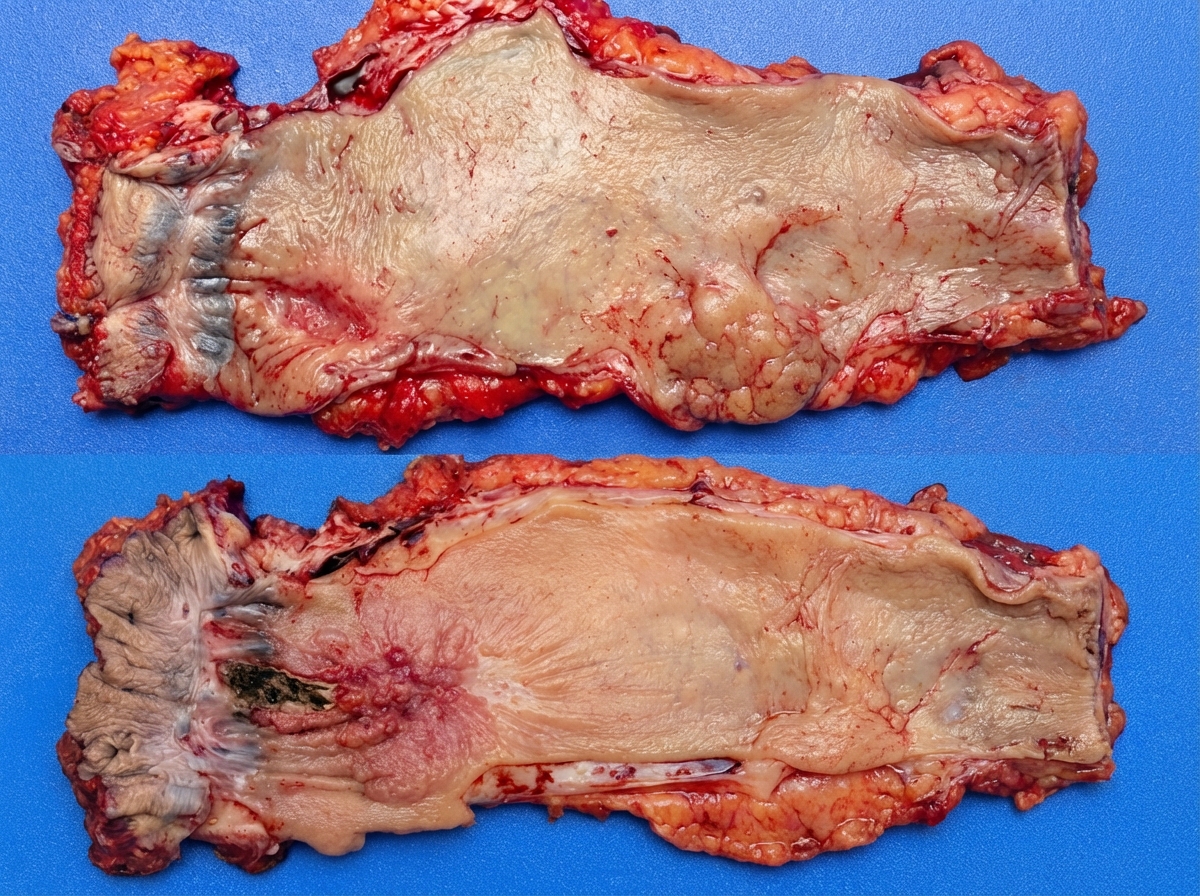
All are correct about the condition shown in the image except: (NEET Pattern 2018)
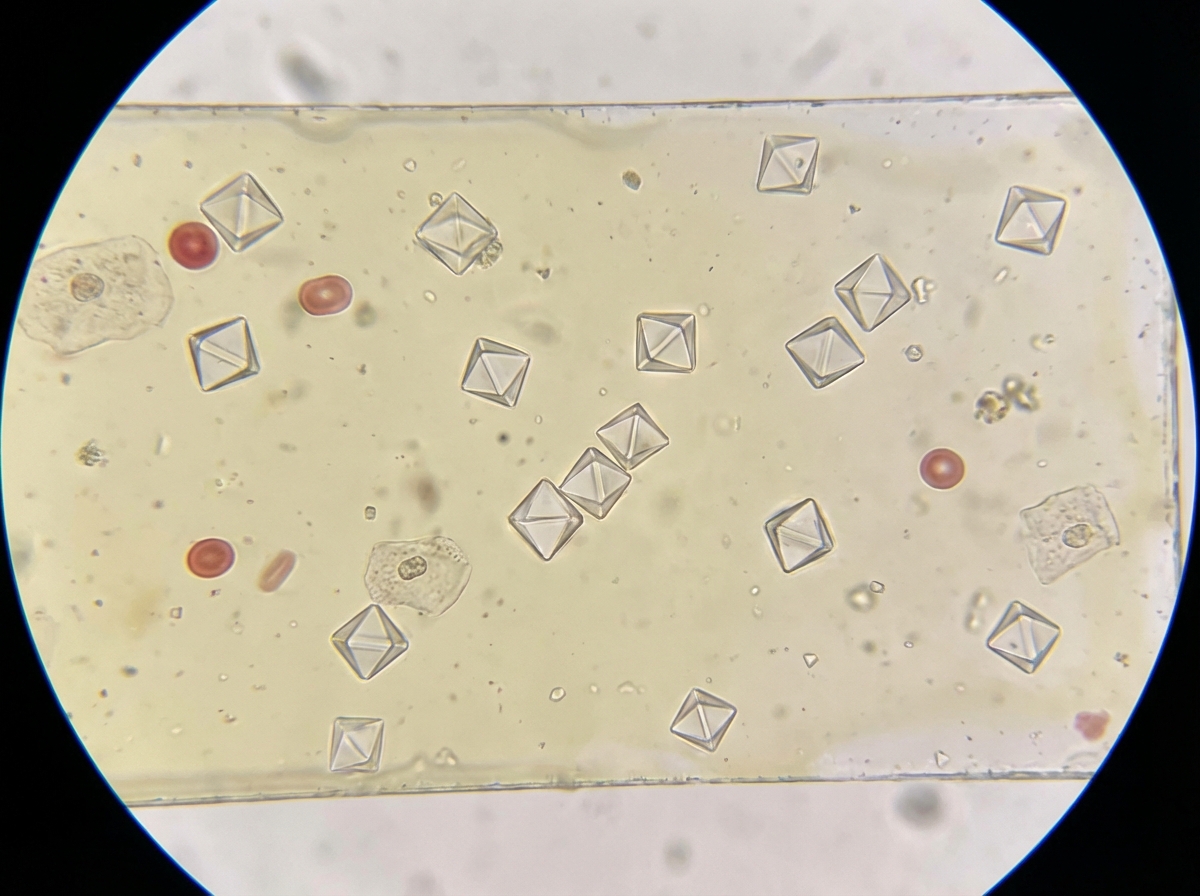
Which urine crystals are shown in the figure below?
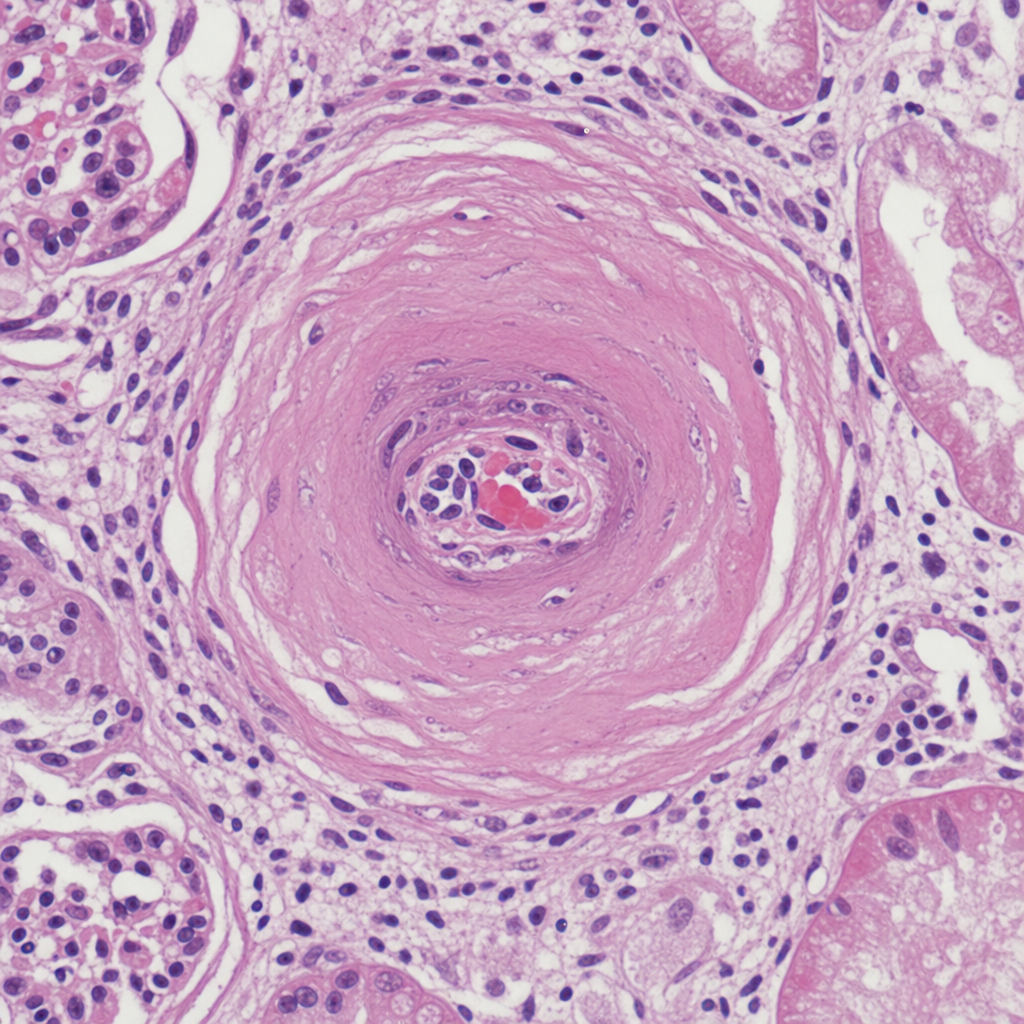
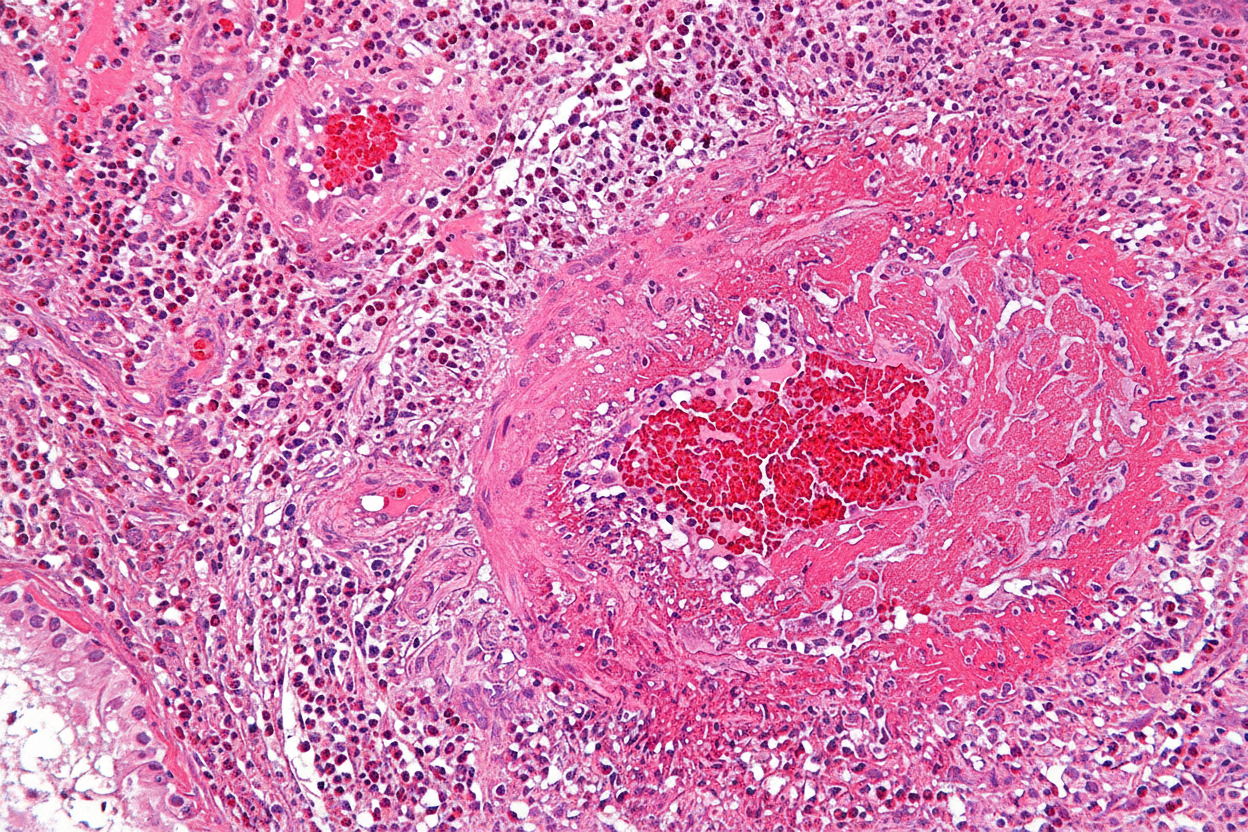
The image shows presence of onion skin proliferation of blood vessels and fibrinoid necrosis visible in
The kidney biopsy image shows presence of:
Practice by Chapter
Congenital renal anomalies
Practice Questions
Glomerular diseases overview
Practice Questions
Nephritic syndrome disorders
Practice Questions
Nephrotic syndrome disorders
Practice Questions
Rapidly progressive glomerulonephritis
Practice Questions
Tubulointerstitial diseases
Practice Questions
Acute tubular necrosis
Practice Questions
Renal vascular diseases
Practice Questions
Pyelonephritis and urinary tract infections
Practice Questions
Renal cystic diseases
Practice Questions
Obstructive uropathies
Practice Questions
Renal tumors
Practice Questions
Kidney transplant pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app