
Pleural diseases — MCQs

A 27-year-old man presents to the emergency department with severe dyspnea and sharp chest pain that suddenly started an hour ago after he finished exercising. He has a history of asthma as a child, and he achieves good control of his acute attacks with Ventolin. On examination, his right lung field is hyperresonant along with diminished lung sounds. Chest wall motion during respiration is asymmetrical. His blood pressure is 105/67 mm Hg, respirations are 22/min, pulse is 78/min, and temperature is 36.7°C (98.0°F). The patient is supported with oxygen, given corticosteroids, and has had analgesic medications via a nebulizer. Considering the likely condition affecting this patient, what is the best step in management?
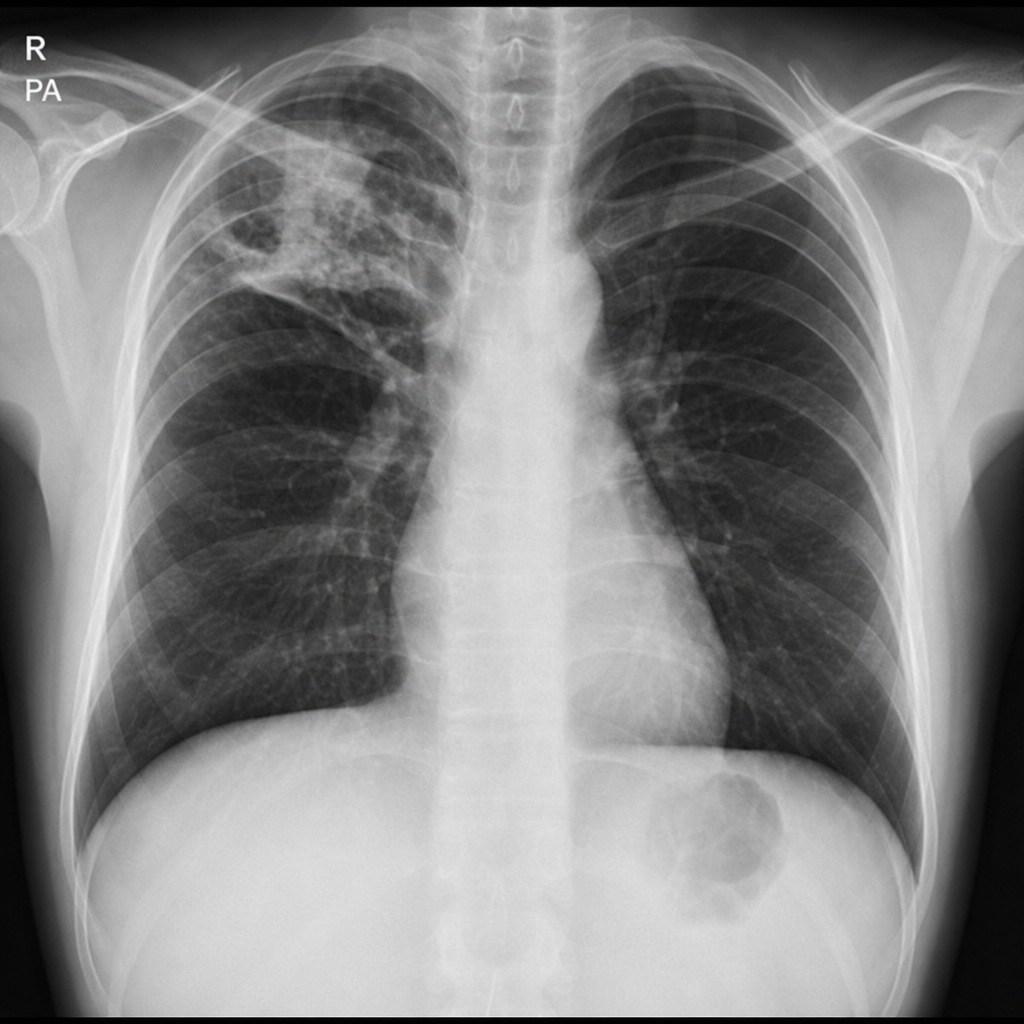
An x-ray of the chest is conducted and shown below. Which of the following is the most appropriate next step in management?
A 61-year-old man comes to the physician because of a 3-month history of worsening exertional dyspnea and a persistent dry cough. For 37 years he has worked in a naval shipyard. He has smoked 1 pack of cigarettes daily for the past 40 years. Pulmonary examination shows fine bibasilar end-expiratory crackles. An x-ray of the chest shows diffuse bilateral infiltrates predominantly in the lower lobes and pleural reticulonodular opacities. A CT scan of the chest shows pleural plaques and subpleural linear opacities. The patient is most likely to develop which of the following conditions?
A 17-year-old boy is brought to the emergency department by his parents 6 hours after he suddenly began to experience dyspnea and pleuritic chest pain at home. He has a remote history of asthma in childhood but has not required any treatment since the age of four. His temperature is 98.4°F (36.9°C), blood pressure is 100/76 mmHg, pulse is 125/min, respirations are 24/min. On exam, he has decreased lung sounds and hyperresonance in the left upper lung field. A chest radiograph shows a slight tracheal shift to the right. What is the best next step in management?
A 72-year-old man presents with shortness of breath and right-sided chest pain. Physical exam reveals decreased breath sounds and dull percussion at the right lung base. Chest X-ray reveals a right-sided pleural effusion. A thoracentesis was performed, removing 450 mL of light pink fluid. Pleural fluid analysis reveals: Pleural fluid to serum protein ratio: 0.35 Pleural fluid to serum LDH ratio: 0.49 Lactate dehydrogenase (LDH): 105 IU (serum LDH Reference: 100–190) Which of the following disorders is most likely in this patient?
A 49-year-old man comes to the hospital for a 10-day history of cough and worsening shortness of breath. He has sharp right-sided chest pain that worsens on inspiration and coughing. Two weeks ago, the patient was admitted to the hospital after passing out on the street from alcohol intoxication but he left against medical advice. He has coronary artery disease and hypertension, and he does not take any medications. He drinks 4 cans of beer daily and has smoked 2 packs of cigarettes daily for 20 years. His temperature is 38.5°C (101.3° F), pulse is 110/min, respirations are 29/min, and blood pressure is 110/65 mmHg. Examination shows poor dentition. There is dullness to percussion at the base of the right lung. Crackles and markedly decreased breath sounds are heard over the right middle and lower lung fields. An x-ray of the chest shows a right-sided loculated pleural effusion and consolidation of the surrounding lung with visible air bronchogram; there are no rib fractures. Thoracocentesis is performed. Examination of this patient's pleural fluid is most likely to show which of the following findings?
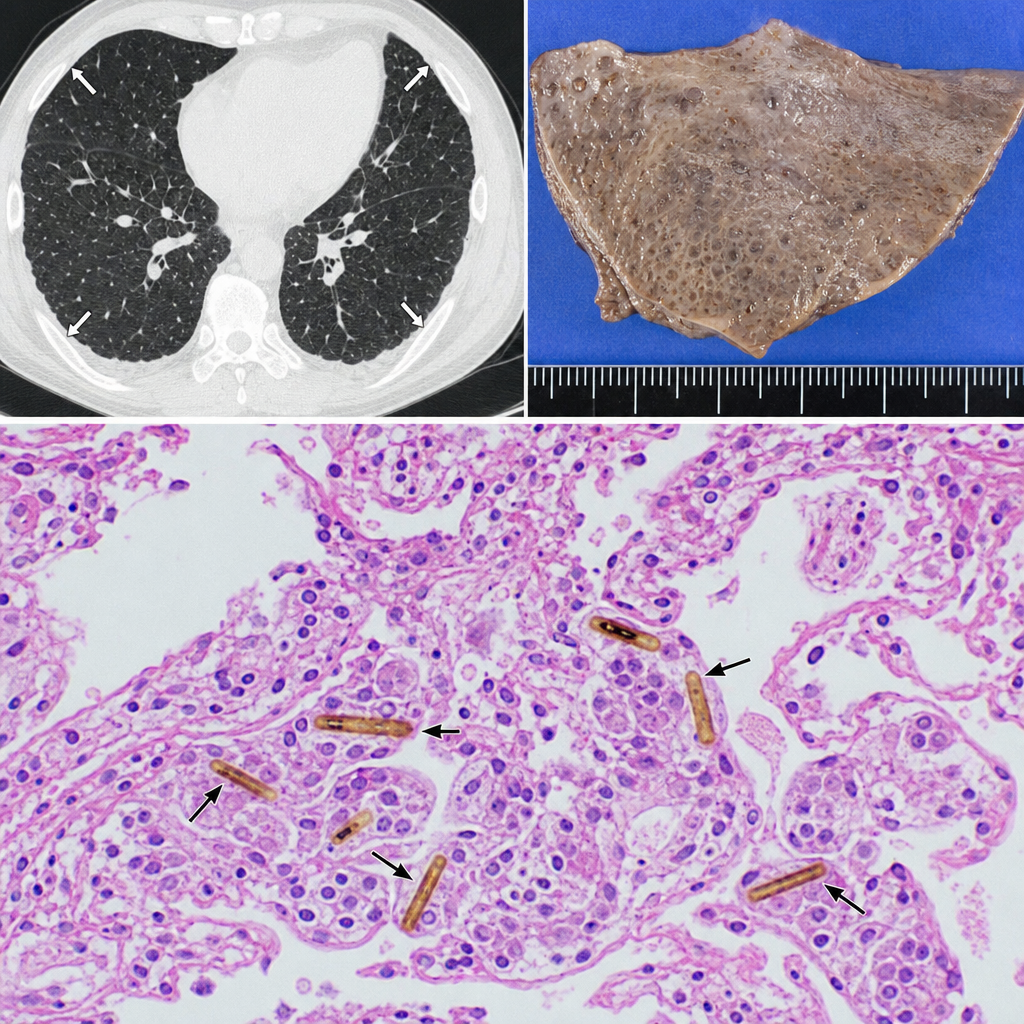
A 58-year-old man with a 40-pack-year smoking history presents with progressive dyspnea and a dry cough. Chest CT reveals bilateral pleural plaques. A wedge biopsy of the lung parenchyma is obtained. Histologic examination reveals elongated, beaded structures with a golden-brown iron-protein coat within macrophages and alveolar spaces, surrounded by mild interstitial fibrosis. Which of the following best describes the structure most characteristic of asbestos exposure identified in this biopsy?
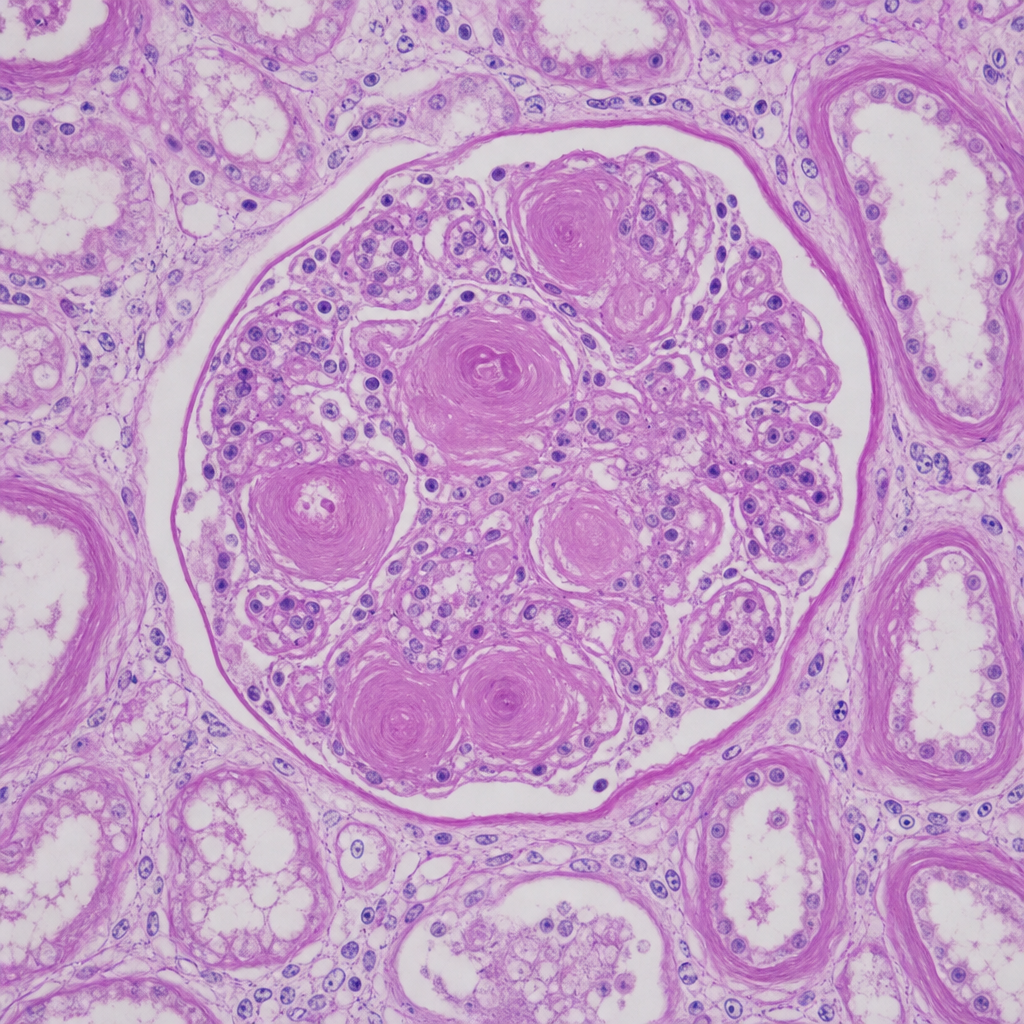
A 67-year-old man with longstanding poorly controlled type 2 diabetes mellitus dies of a myocardial infarction. At autopsy, both kidneys appear symmetrically shrunken with granular surfaces. A PAS-stained section of renal cortex at 20× magnification shows ovoid, laminated, acellular deposits within the mesangium of glomeruli, compressing the capillary loops. The tubular basement membranes are markedly thickened. Which of the following best characterizes the composition and pathogenetic mechanism of the glomerular deposits shown?
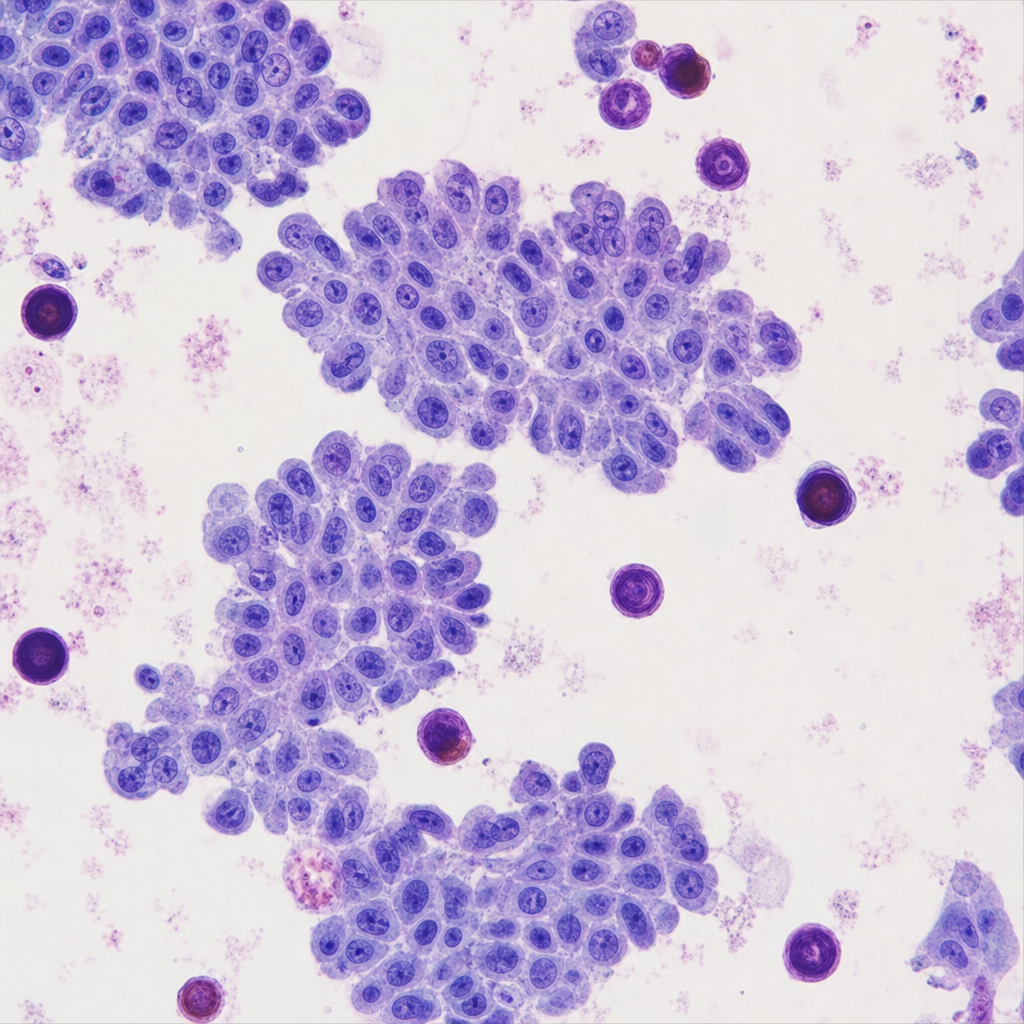
A 45-year-old woman presents with a 3-cm solitary thyroid nodule. Fine-needle aspiration is performed. The cytology reveals cells arranged in papillary clusters with enlarged nuclei exhibiting longitudinal grooves, pale 'ground-glass' chromatin, and intranuclear cytoplasmic pseudoinclusions. Scattered in the smear/background and within papillary fragments are laminated calcified spherules. Which of the following eponymous structures are represented by those calcified deposits, and in which additional neoplasm are identical structures characteristically found?
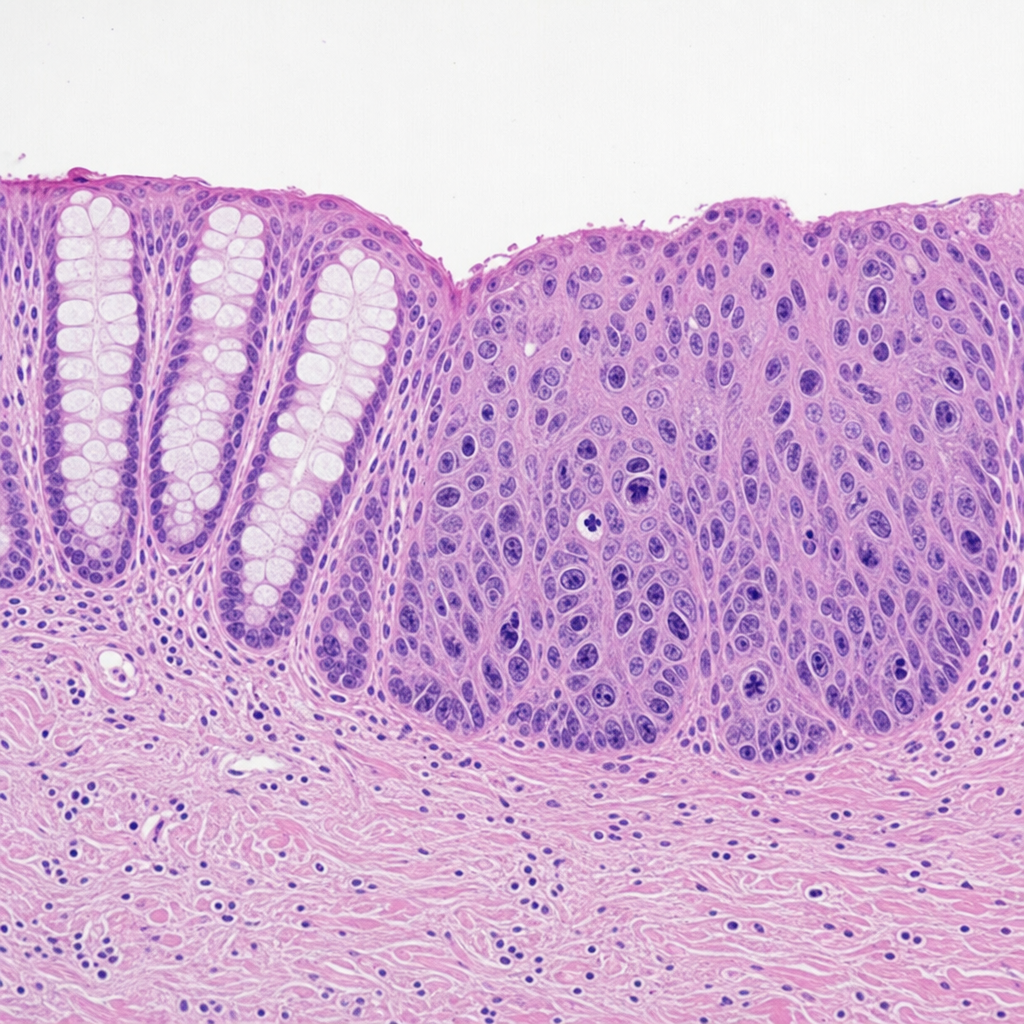
A 55-year-old woman with a history of Barrett esophagus undergoes surveillance endoscopy. A 1.5 cm nodular lesion is identified in the distal esophagus and biopsied. The photomicrograph shows glandular epithelium with marked nuclear enlargement, prominent nucleoli, loss of polarity, and atypical mitoses. The abnormal cells are confined to the epithelium above an intact basement membrane with no stromal invasion. The adjacent non-dysplastic mucosa shows columnar epithelium with goblet cells. Which of the following best characterizes the biological behavior and reversibility of the lesion depicted in this biopsy?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app