
Pulmonary — MCQs

On this page
A 61-year-old male presents to your office with fever and dyspnea on exertion. He has been suffering from chronic, non-productive cough for 1 year. You note late inspiratory crackles on auscultation. Pulmonary function tests reveal an FEV1/FVC ratio of 90% and an FVC that is 50% of the predicted value. Which of the following would you most likely see on a biopsy of this patient's lung?
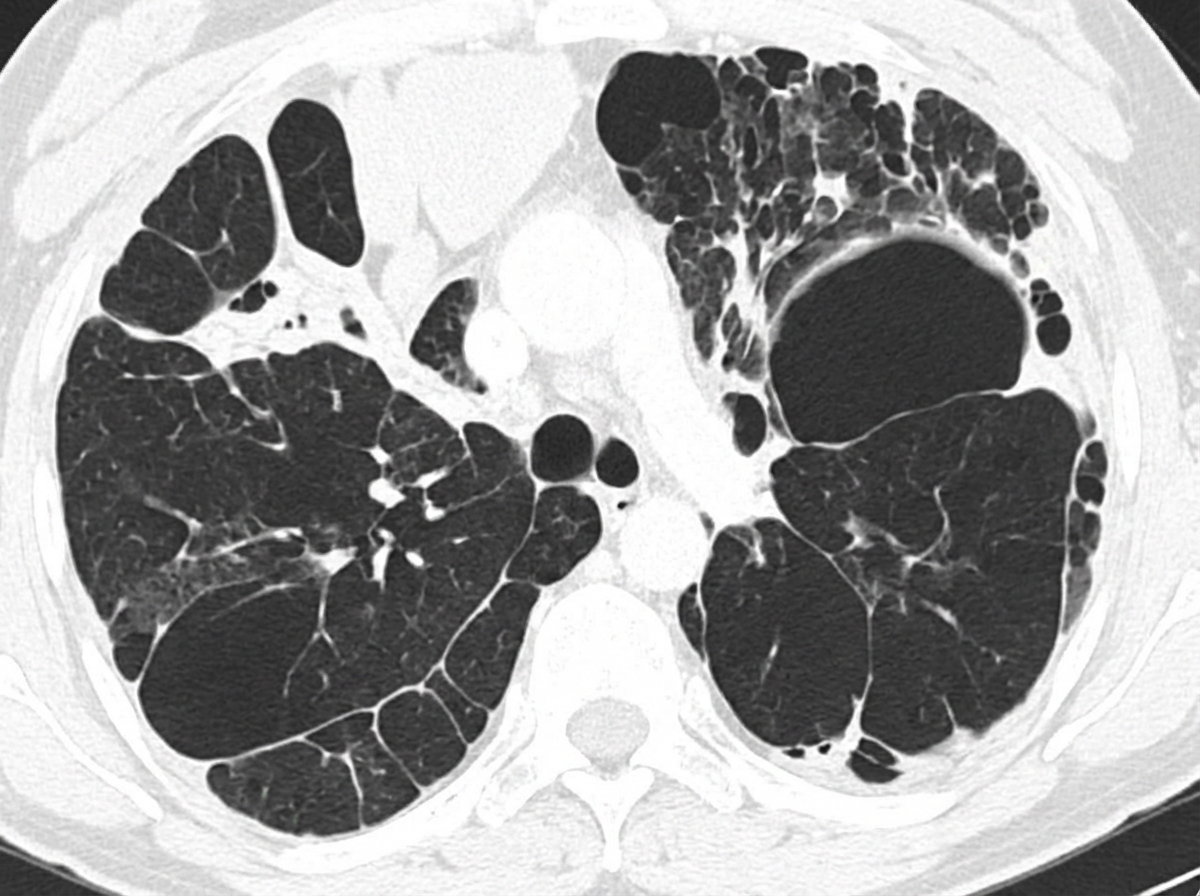
A 58-year-old woman presents to the physician with a cough that began 6 years ago, as well as intermittent difficulty in breathing for the last year. There is no significant sputum production. There is no history of rhinorrhea, sneezing or nose congestion. She has been a chronic smoker from early adulthood. Her temperature is 36.9°C (98.4°F), the heart rate is 80/min, the blood pressure is 128/84 mm Hg, and the respiratory rate is 22/min. A physical examination reveals diffuse end-expiratory wheezing with prolonged expiration on chest auscultation; breath sounds and heart sounds are diminished. There is no cyanosis, clubbing or lymphadenopathy. Her chest radiogram shows hyperinflated lungs bilaterally and a computed tomography scan of her chest is shown in the picture. Which of the following best describes the pathogenesis of the condition of this patient?
A 32-year-old man comes to the physician for a 1-month history of fever, chest pain with deep breathing, and a 4-kg (9 lb) weight loss. His temperature is 38°C (100.4°F). An x-ray of the chest shows a subpleural nodule in the right lower lobe with right hilar lymphadenopathy. Histological examination of a right hilar lymph node biopsy specimen shows several granulomas with acellular cores. Which of the following is the most likely diagnosis?
An investigator is studying the effects of influenza virus on human lung tissue. Biopsy specimens of lung parenchyma are obtained from patients recovering from influenza pneumonia and healthy control subjects. Compared to the lung tissue from the healthy control subjects, the lung tissue from the affected patients is most likely to show which of the following findings on histopathologic examination?
A lung mass of a 50 pack-year smoker is biopsied. If ADH levels were grossly increased, what would most likely be the histologic appearance of this mass?
A 73-year-old man is brought to the emergency department because of fever, malaise, dyspnea, and a productive cough with purulent sputum for the past day. His temperature is 39.2°C (102.6°F). Pulmonary examination shows crackles over the right upper lung field. Sputum Gram stain shows gram-positive cocci. Despite the appropriate treatment, the patient dies 5 days later. At autopsy, gross examination shows that the right lung has a pale, grayish-brown appearance and a firm consistency. Microscopic examination of the tissue is most likely to show which of the following?
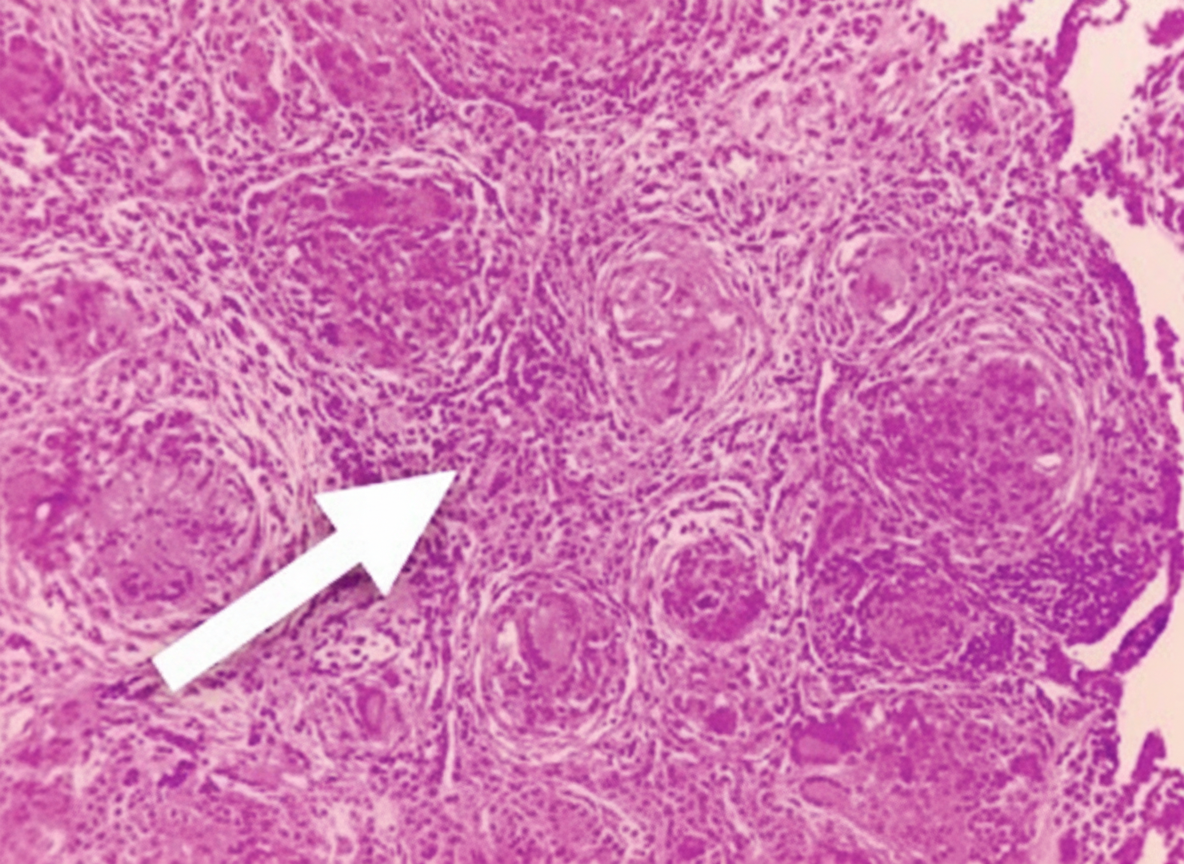
A 38-year-old man comes to the physician because of fever, malaise, cough, and shortness of breath for 2 months. He has had a 4-kg (9-lb) weight loss during the same period. He works at a flour mill and does not smoke cigarettes. His temperature is 38.1°C (100.6°F) and pulse oximetry shows 95% on room air. Diffuse fine crackles are heard over both lung fields. A chest x-ray shows patchy reticulonodular infiltrates in the mid and apical lung fields bilaterally. A photomicrograph of a lung biopsy specimen is shown. Which of the following cytokines have the greatest involvement in the pathogenesis of the lesion indicated by the arrow?
A 61-year-old man presents with gradually increasing shortness of breath. For the last 2 years, he has had a productive cough on most days. Past medical history is significant for hypertension and a recent admission to the hospital for pneumonia. He uses a triamcinolone inhaler and uses an albuterol inhaler as a rescue inhaler. He also takes lisinopril and a multivitamin daily. He has smoked a pack a day for the last 32 years and has no intention to quit now. Today, his blood pressure is 142/97 mm Hg, heart rate is 97/min, respiratory rate is 22/min, and temperature is 37.4°C (99.3°F). On physical exam, he has tachypnea and has some difficulty finishing his sentences. His heart has a regular rate and rhythm. Auscultation of his lungs reveals wheezing and rhonchi that improves after a deep cough. Fremitus is absent. Pulmonary function tests show FEV1/FVC of 55% with no change in FEV1 after albuterol treatment. Which of the following is the most likely pathology associated with this patient's disease?
A 53-year-old man is admitted to the intensive care unit from the emergency department with severe pancreatitis. Overnight, he starts to develop severe hypoxemia, and he is evaluated by a rapid response team. On exam the patient is breathing very quickly and has rales and decreased breath sounds bilaterally. He is placed on 50% FiO2, and an arterial blood gas is collected with the following results: pH: 7.43 pCO2: 32 mmHg pO2: 78 mmHg The oxygen status of the patient continues to deteriorate, and he is placed on ventilator support. Which of the following would most likely be seen in this patient?
A 73-year-old female with no past medical history is hospitalized after she develops a fever associated with increasing shortness of breath. She states that 1 week prior, she had a cold which seemed to be resolving. Yesterday, however, she noticed that she started to feel feverish, measured her temperature to be 101.5°F (38.6°C), and also developed an unproductive dry cough and difficulty breathing. On exam, her temperature is 100.8°F (38.2°C), blood pressure is 110/72 mmHg, pulse is 96/min, and respirations are 16/min. Her exam demonstrates decreased breath sounds at the right lung base. The chest radiograph shows a right-sided pleural effusion with an opacity in the right lower lobe that is thought to be a bacterial pneumonia. Which of the following can be expected on a sample of the effusion fluid?
Practice by Chapter
Atelectasis
Practice Questions
Pulmonary edema
Practice Questions
Acute respiratory distress syndrome
Practice Questions
Obstructive lung diseases (emphysema, bronchitis)
Practice Questions
Asthma pathology
Practice Questions
Bronchiectasis
Practice Questions
Restrictive lung diseases
Practice Questions
Interstitial lung diseases
Practice Questions
Pulmonary vascular disorders
Practice Questions
Pulmonary infections
Practice Questions
Lung tumors (primary and metastatic)
Practice Questions
Pleural diseases
Practice Questions
Congenital lung anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app