
Pulmonary — MCQs

On this page
An investigator is studying early post-mortem changes in the lung. Autopsies are performed on patients who died following recent hospital admissions. Microscopic examination of the lungs at one of the autopsies shows numerous macrophages with brown intracytoplasmic inclusions. A Prussian blue stain causes these inclusions to turn blue. These findings are most consistent with a pathological process that would manifest with which of the following symptoms?
A 65-year-old male presented to his primary care physician with exertional dyspnea. The patient had a 30-year history of smoking one pack of cigarettes per day. Physical examination reveals a barrel-chested appearance, and it is noted that the patient breathes through pursed lips. Spirometry shows decreased FEV1, FVC, and FEV1/FVC. This patient’s upper lobes are most likely to demonstrate which of the following?
A 55-year-old woman comes to the physician with a 6-month history of cough and dyspnea. She has smoked 1 pack of cigarettes daily for the past 30 years. Analysis of the sputum sample from bronchoalveolar lavage shows abnormal amounts of an isoform of elastase that is normally inhibited by alpha-1 antitrypsin. The cell responsible for secreting this elastase is most likely also responsible for which of the following functions?
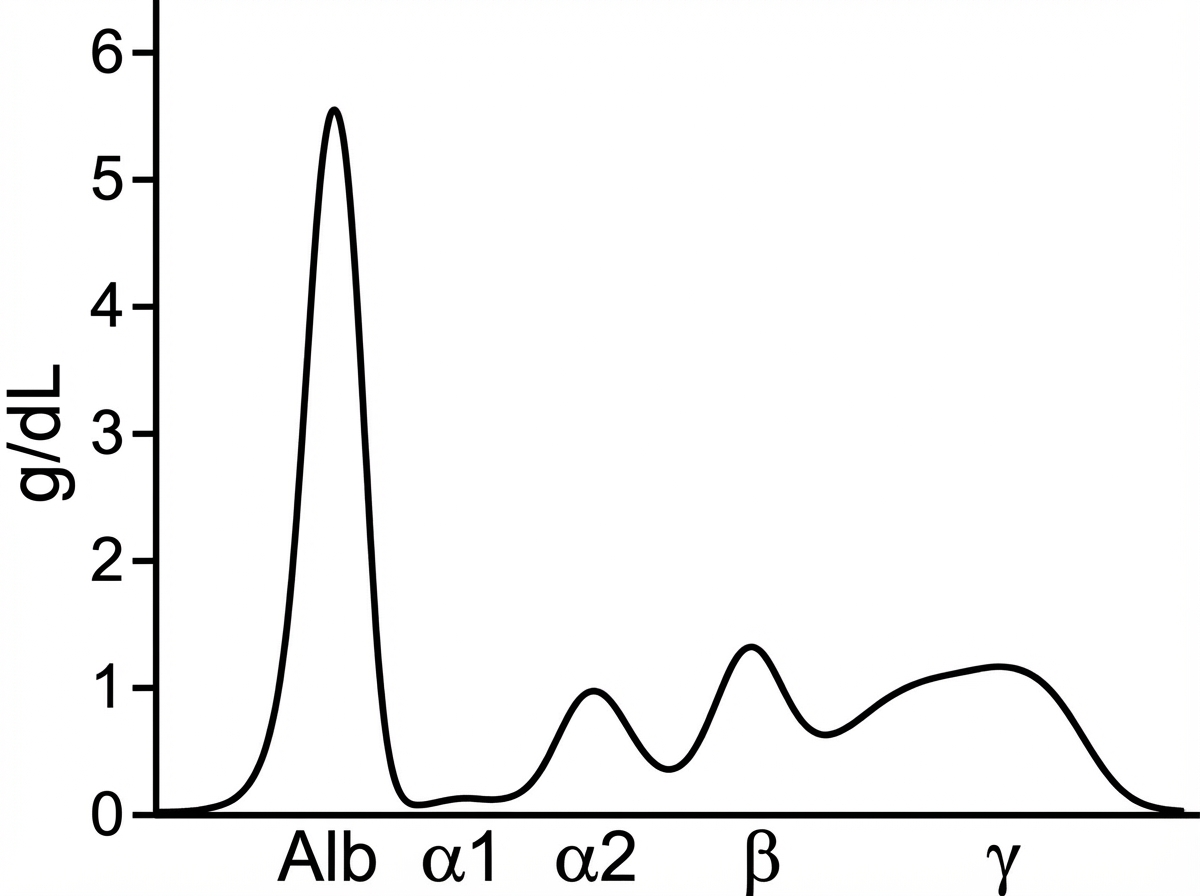
A 13-year-old boy is brought to the emergency department with respiratory distress, fever, and a productive cough. Past medical history is significant for a history of recurrent bronchopneumonia since the age of 5, managed conservatively with antibiotics and mucolytic therapy. The patient's weight was normal at birth, but he suffered from a failure to thrive, although there was no neonatal history of chronic diarrhea or jaundice. His current vitals are a respiratory rate of 26/min, a pulse of 96/min, a temperature of 38.8℃ (101.8°F), a blood pressure of 90/60 mm Hg, and oxygen saturation of 88% on room air. On physical examination, there is coarse crepitus bilaterally and both expiratory and inspiratory wheezing is present. The chest radiograph shows evidence of diffuse emphysema. A sweat chloride test and nitroblue tetrazolium test are both within normal limits. A complete blood count is significant for the following: WBC 26300/mm3 Neutrophils 62% Lymphocytes 36% Eosinophils 2% Total bilirubin 0.8 mg/dL Direct bilirubin 0.2 mg/dL SGOT 100 U/L SGPT 120 U/L ALP 200 U/L Results of serum protein electrophoresis are shown in the figure. Which of the following is the most likely diagnosis in this patient?
A 15-year-old boy is brought to the emergency department with a 30 minute history of difficulty breathing. He was playing basketball in gym class when he suddenly felt pain in the right side of his chest that got worse when he tried to take a deep breath. Physical exam reveals a tall, thin boy taking rapid shallow breaths. There are decreased breath sounds in the right lung fields and the right chest is hyperresonant to percussion. Which of the following is true of the lesions that would most likely be seen in this patient's lungs?
A 56-year-old man comes to the physician for a follow-up examination one week after a chest x-ray showed a solitary pulmonary nodule. He has no history of major medical illness. He has smoked 1 pack of cigarettes daily for the past 30 years. Physical examination shows no abnormalities. A tuberculin skin test is negative. A CT scan of the chest shows a 2.1-cm well-circumscribed, calcified nodule in the periphery of the right lower lung field. A CT-guided biopsy of the lesion is performed. Histological examination of the biopsy specimen shows regions of disorganized hyaline cartilage interspersed with myxoid regions and clefts of ciliated epithelium. Which of the following is the most likely diagnosis?
A 72-year-old retired shipyard worker received a chest x-ray as part of a routine medical work-up. The radiologist reported incidental findings suggestive of an occupational lung disease. Which of the following descriptions is most consistent with this patient's film?
A 66-year-old man presents with severe respiratory distress. He was diagnosed with pulmonary hypertension secondary to occupational pneumoconiosis. Biopsy findings of the lung showed ferruginous bodies. What is the most likely etiology?
A 58-year-old man is brought to the emergency department after a witnessed tonic-clonic seizure. His wife says he has had a persistent dry cough for 6 months. During this time period, he has also had fatigue and a 4.5-kg (10-lb) weight loss. The patient has no history of serious illness and does not take any medications. He has smoked 1 pack of cigarettes daily for 35 years. He is confused and oriented only to person. Laboratory studies show a serum sodium concentration of 119 mEq/L and glucose concentration of 102 mg/dL. An x-ray of the chest shows an irregular, poorly demarcated density at the right hilum. Microscopic examination of this density is most likely to confirm which of the following diagnoses?
A 68-year-old man presents to the office with progressive shortness of breath and cough. A chest X-ray shows prominent hilar lymph nodes and scattered nodular infiltrates. Biopsy of the latter reveals noncaseating granulomas. This patient most likely has a history of exposure to which of the following?
Practice by Chapter
Atelectasis
Practice Questions
Pulmonary edema
Practice Questions
Acute respiratory distress syndrome
Practice Questions
Obstructive lung diseases (emphysema, bronchitis)
Practice Questions
Asthma pathology
Practice Questions
Bronchiectasis
Practice Questions
Restrictive lung diseases
Practice Questions
Interstitial lung diseases
Practice Questions
Pulmonary vascular disorders
Practice Questions
Pulmonary infections
Practice Questions
Lung tumors (primary and metastatic)
Practice Questions
Pleural diseases
Practice Questions
Congenital lung anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app