
Interstitial lung diseases — MCQs

A 61-year-old male presents to your office with fever and dyspnea on exertion. He has been suffering from chronic, non-productive cough for 1 year. You note late inspiratory crackles on auscultation. Pulmonary function tests reveal an FEV1/FVC ratio of 90% and an FVC that is 50% of the predicted value. Which of the following would you most likely see on a biopsy of this patient's lung?
A 68-year-old man presents to the office with progressive shortness of breath and cough. A chest X-ray shows prominent hilar lymph nodes and scattered nodular infiltrates. Biopsy of the latter reveals noncaseating granulomas. This patient most likely has a history of exposure to which of the following?
A 35-year-old female comes to the physician because of a 2-year history of progressive fatigue and joint pain. She has a 1-year history of skin problems and a 4-month history of episodic pallor of her fingers. She reports that the skin of her face, neck, and hands is always dry and itchy; there are also numerous “red spots” on her face. She has become more “clumsy” and often drops objects. She has gastroesophageal reflux disease treated with lansoprazole. She does not smoke. She occasionally drinks a beer or a glass of wine. Her temperature is 36.5°C (97.7°F), blood pressure is 154/98 mm Hg, and pulse is 75/min. Examination shows hardening and thickening of the skin of face, neck, and hands. There are small dilated blood vessels around her mouth and on her oral mucosa. Mouth opening is reduced. Active and passive range of motion of the proximal and distal interphalangeal joints is limited. Cardiopulmonary examination shows no abnormalities. Her creatinine is 1.4 mg/dL. The patient is at increased risk for which of the following complications?
A 37-year-old woman comes to the physician because of a 10-month history of excessive daytime sleepiness and fatigue. She says she has difficulty concentrating and has fallen asleep at work on numerous occasions. She also reports having frequent headaches during the day. She has no difficulty falling asleep at night, but wakes up gasping for breath at least once. She has always snored loudly and began using an oral device to decrease her snoring a year ago. She has occasional lower back pain, for which she takes tramadol tablets 1–2 times per week. She also began taking one rabeprazole tablet daily 3 weeks ago. She does not smoke. She is 175 cm (5 ft 7 in) tall and weighs 119 kg (262 lb); BMI is 38.8 kg/m2. Her vital signs are within normal limits. Physical and neurologic examinations show no other abnormalities. Arterial blood gas analysis on room air shows: pH 7.35 PCO2 51 mm Hg PO2 64 mm Hg HCO3- 29 mEq/L O2 saturation 92% An x-ray of the chest and ECG show no abnormalities. Which of the following is the most likely cause of this patient's condition?
A 49-year-old woman comes to the physician because of a 4-month history of a dry cough and shortness of breath on exertion. She also reports recurrent episodes of pain, stiffness, and swelling in her wrist and her left knee over the past 6 months. She had two miscarriages at age 24 and 28. Physical examination shows pallor, ulcerations on the palate, and annular hyperpigmented plaques on the arms and neck. Fine inspiratory crackles are heard over bilateral lower lung fields on auscultation. Which of the following additional findings is most likely in this patient?
A 62-year-old man presents to the emergency department for evaluation of a 2-year history of increasing shortness of breath. He also has an occasional nonproductive cough. The symptoms get worse with exertion. The medical history is significant for hypertension and he takes chlorthalidone. He is a smoker with a 40-pack-year smoking history. On physical examination, the patient is afebrile; the vital signs include: blood pressure 125/78 mm Hg, pulse 90/min, and respiratory rate 18/min. The body mass index (BMI) is 31 kg/m2. The oxygen saturation is 94% at rest on room air. A pulmonary examination reveals decreased breath sounds bilaterally, but is otherwise normal with no wheezes or crackles. The remainder of the examination is unremarkable. A chest radiograph shows hyperinflation of both lungs with mildly increased lung markings, but no focal findings. Based on this clinical presentation, which of the following is most likely?
A 31 year-old African-American female presents with painful shin nodules, uveitis, and calcified hilar lymph nodes. A transbronchial biopsy of the lung would most likely show which of the following histologies?
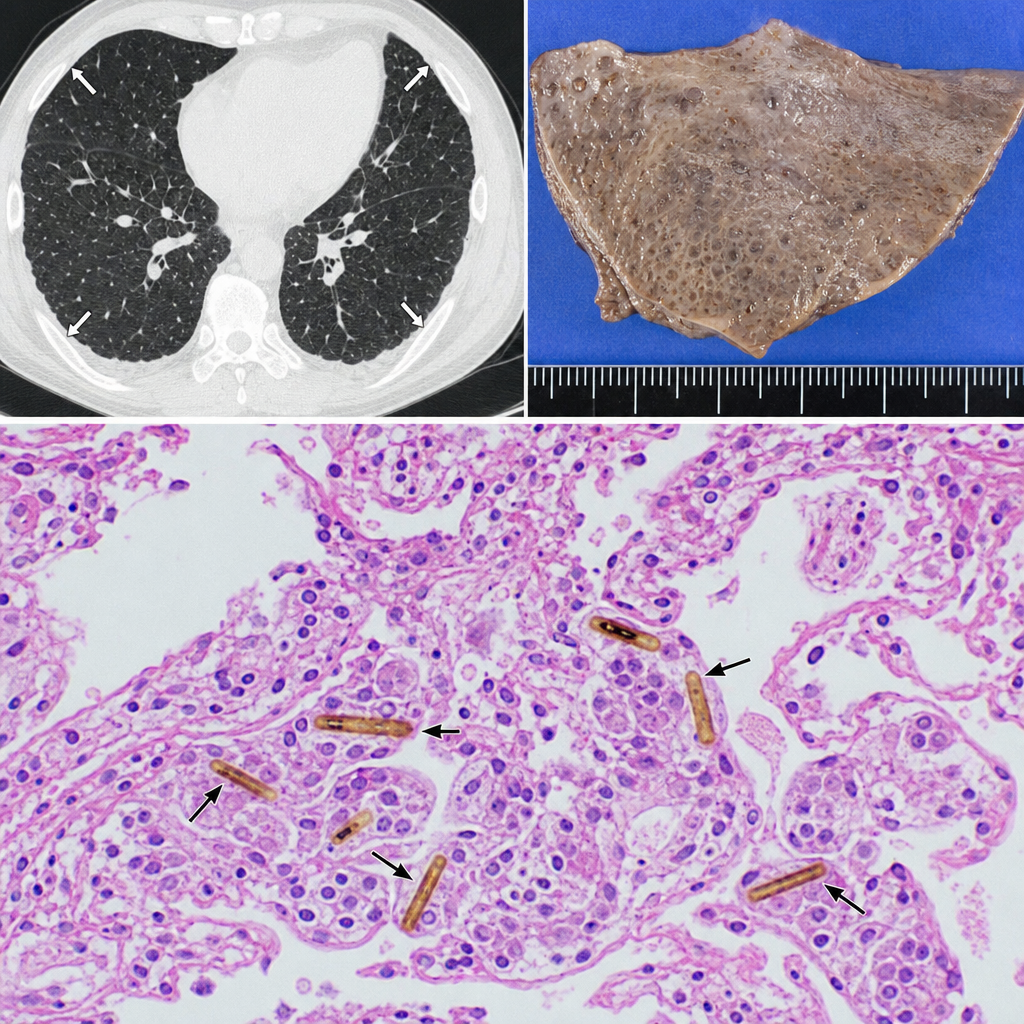
A 58-year-old man with a 40-pack-year smoking history presents with progressive dyspnea and a dry cough. Chest CT reveals bilateral pleural plaques. A wedge biopsy of the lung parenchyma is obtained. Histologic examination reveals elongated, beaded structures with a golden-brown iron-protein coat within macrophages and alveolar spaces, surrounded by mild interstitial fibrosis. Which of the following best describes the structure most characteristic of asbestos exposure identified in this biopsy?
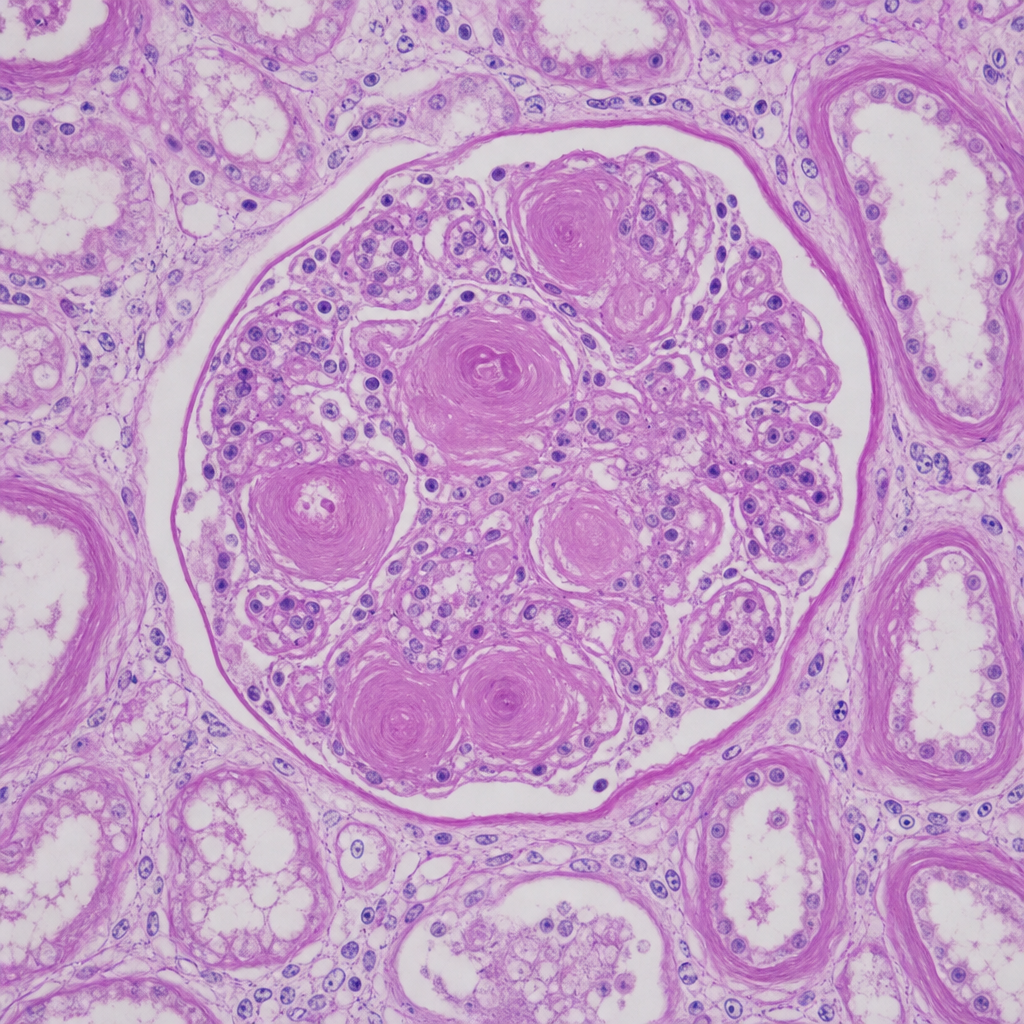
A 67-year-old man with longstanding poorly controlled type 2 diabetes mellitus dies of a myocardial infarction. At autopsy, both kidneys appear symmetrically shrunken with granular surfaces. A PAS-stained section of renal cortex at 20× magnification shows ovoid, laminated, acellular deposits within the mesangium of glomeruli, compressing the capillary loops. The tubular basement membranes are markedly thickened. Which of the following best characterizes the composition and pathogenetic mechanism of the glomerular deposits shown?
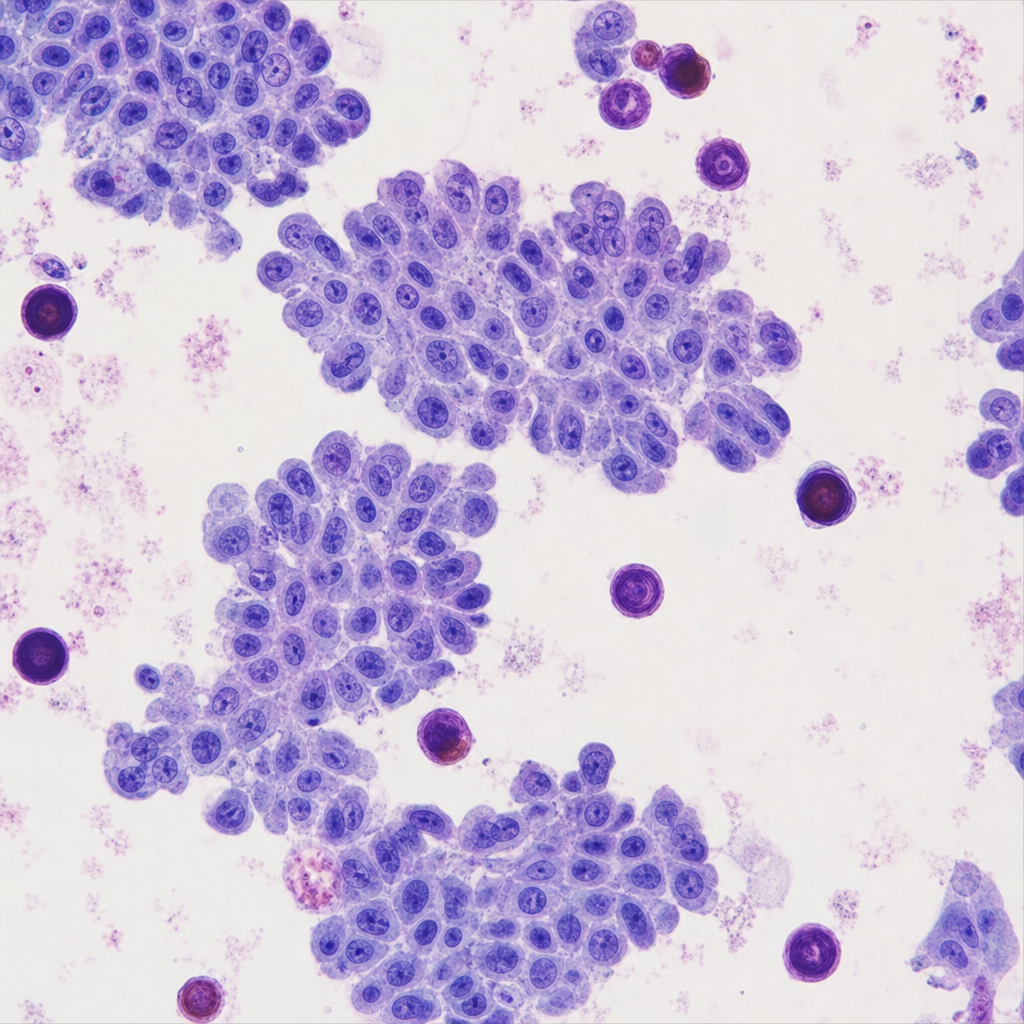
A 45-year-old woman presents with a 3-cm solitary thyroid nodule. Fine-needle aspiration is performed. The cytology reveals cells arranged in papillary clusters with enlarged nuclei exhibiting longitudinal grooves, pale 'ground-glass' chromatin, and intranuclear cytoplasmic pseudoinclusions. Scattered in the smear/background and within papillary fragments are laminated calcified spherules. Which of the following eponymous structures are represented by those calcified deposits, and in which additional neoplasm are identical structures characteristically found?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app