
Pulmonary — MCQs

On this page
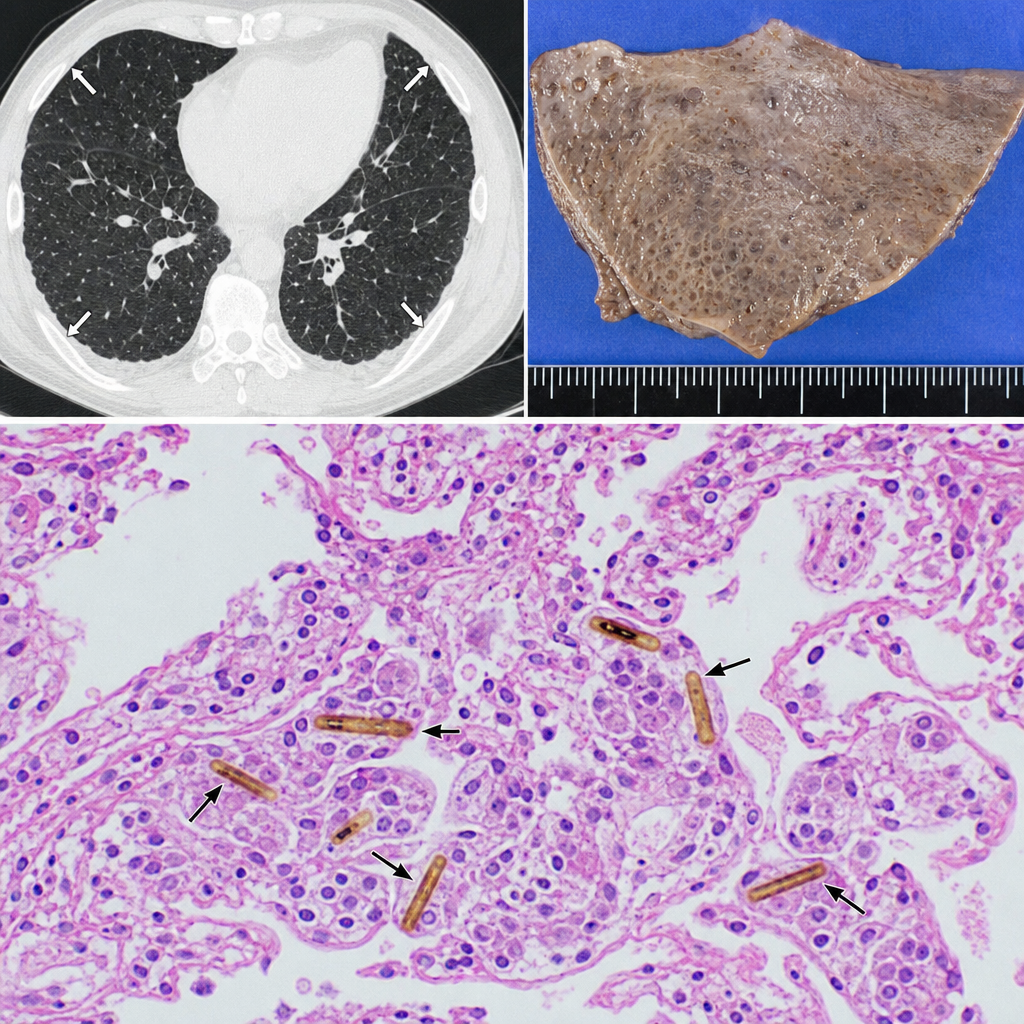
A 58-year-old man with a 40-pack-year smoking history presents with progressive dyspnea and a dry cough. Chest CT reveals bilateral pleural plaques. A wedge biopsy of the lung parenchyma is obtained. Histologic examination reveals elongated, beaded structures with a golden-brown iron-protein coat within macrophages and alveolar spaces, surrounded by mild interstitial fibrosis. Which of the following best describes the structure most characteristic of asbestos exposure identified in this biopsy?
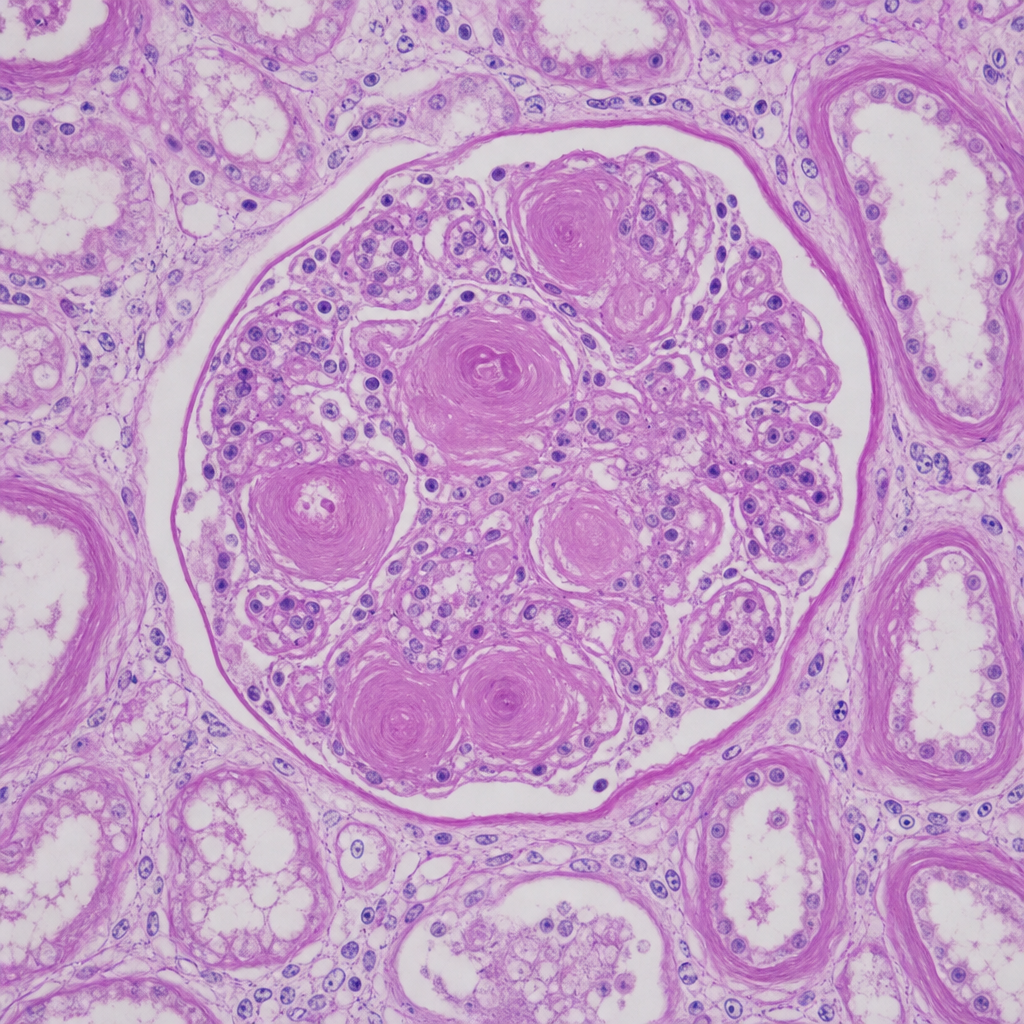
A 67-year-old man with longstanding poorly controlled type 2 diabetes mellitus dies of a myocardial infarction. At autopsy, both kidneys appear symmetrically shrunken with granular surfaces. A PAS-stained section of renal cortex at 20× magnification shows ovoid, laminated, acellular deposits within the mesangium of glomeruli, compressing the capillary loops. The tubular basement membranes are markedly thickened. Which of the following best characterizes the composition and pathogenetic mechanism of the glomerular deposits shown?
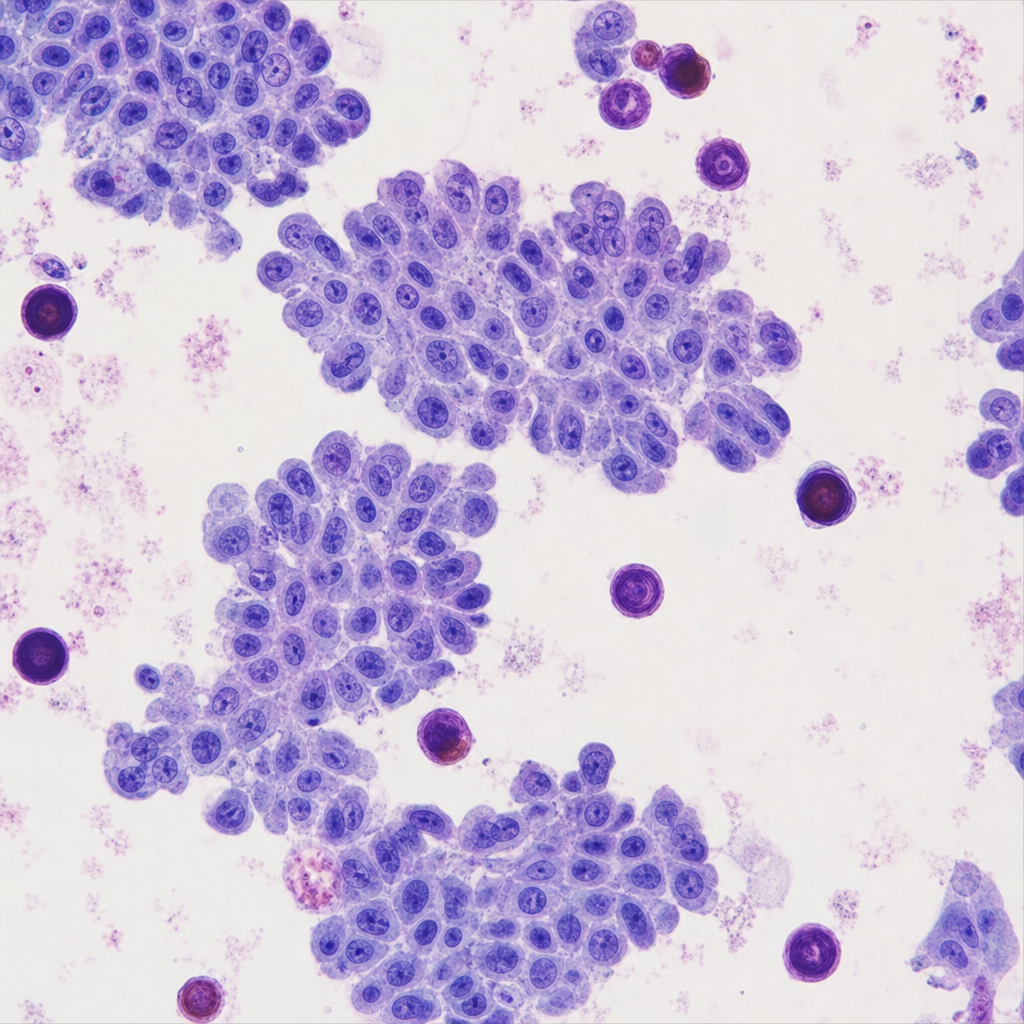
A 45-year-old woman presents with a 3-cm solitary thyroid nodule. Fine-needle aspiration is performed. The cytology reveals cells arranged in papillary clusters with enlarged nuclei exhibiting longitudinal grooves, pale 'ground-glass' chromatin, and intranuclear cytoplasmic pseudoinclusions. Scattered in the smear/background and within papillary fragments are laminated calcified spherules. Which of the following eponymous structures are represented by those calcified deposits, and in which additional neoplasm are identical structures characteristically found?
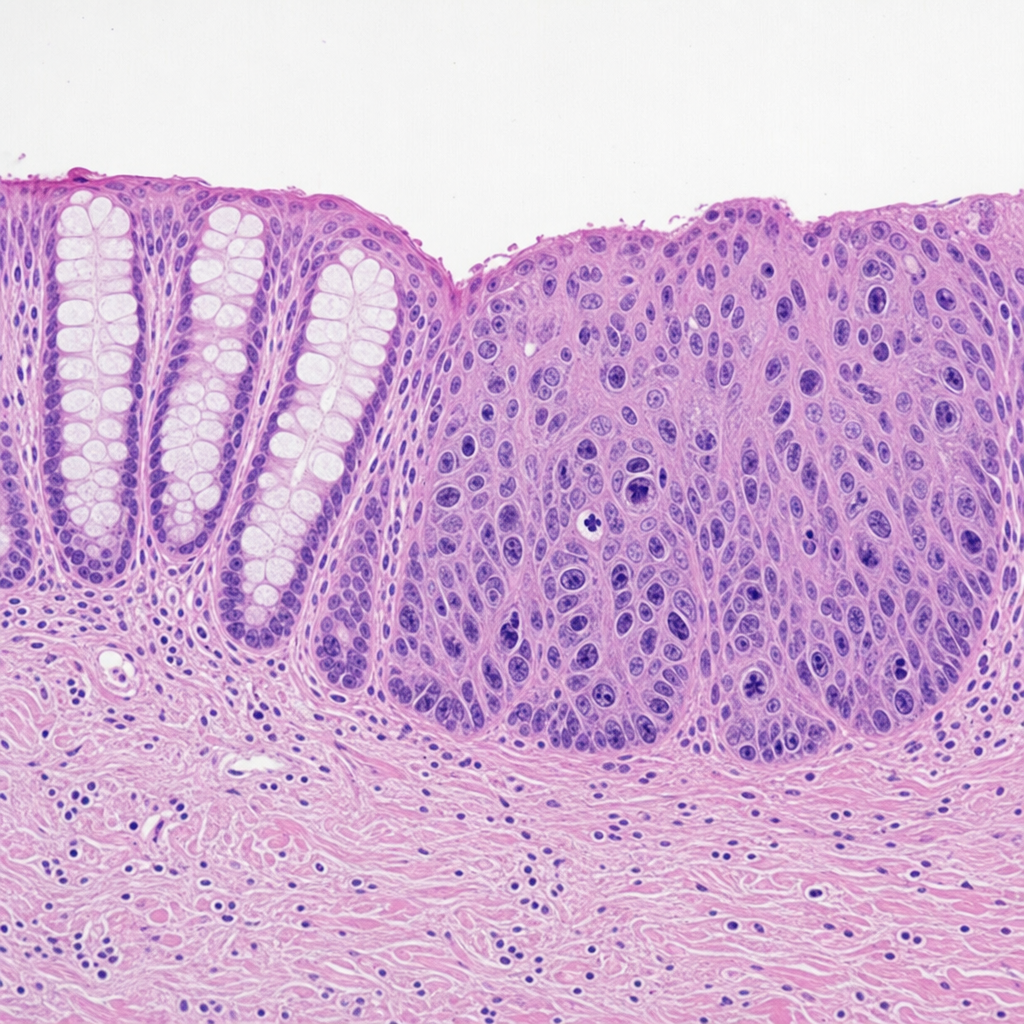
A 55-year-old woman with a history of Barrett esophagus undergoes surveillance endoscopy. A 1.5 cm nodular lesion is identified in the distal esophagus and biopsied. The photomicrograph shows glandular epithelium with marked nuclear enlargement, prominent nucleoli, loss of polarity, and atypical mitoses. The abnormal cells are confined to the epithelium above an intact basement membrane with no stromal invasion. The adjacent non-dysplastic mucosa shows columnar epithelium with goblet cells. Which of the following best characterizes the biological behavior and reversibility of the lesion depicted in this biopsy?
A 31 year-old African-American female presents with painful shin nodules, uveitis, and calcified hilar lymph nodes. A transbronchial biopsy of the lung would most likely show which of the following histologies?
A 68-year-old male smoker dies suddenly in a car accident. He had smoked 2 packs per day for 40 years. His past medical history is notable for a frequent, very productive cough, recurrent respiratory infections and occasional wheezing. He had no other medical problems. At autopsy, which of the following is most likely to be found in this patient?
A 44-year-old man comes to the physician because of a 5-month history of persistent cough productive of thick, yellow sputum and worsening shortness of breath. One year ago, he had similar symptoms that lasted 4 months. He has smoked two packs of cigarettes daily for the past 20 years. Physical examination shows scattered expiratory wheezing and rhonchi throughout both lung fields. Microscopic examination of a lung biopsy specimen is most likely to show which of the following findings?
A 63-year-old man with alpha-1-antitrypsin deficiency is brought to the emergency department 1 hour after his daughter found him unresponsive. Despite appropriate care, the patient dies. At autopsy, examination of the lungs shows enlargement of the airspaces in the respiratory bronchioles and alveoli. Enzymatic activity of which of the following cells is the most likely cause of these findings?
A 60-year-old man who is a chronic smoker comes to the hospital with the chief complaint of shortness of breath which has worsened over the past 2 days. He also has a productive cough with yellowish sputum. There is no history of hemoptysis, chest pain, fever, palpitations, or leg swelling. He had a viral illness one week ago. He has been using an inhaler for 10 years for his respiratory disease. He sleeps with 2 pillows every night. He received 100 mg of hydrocortisone and antibiotics in the emergency department, and his symptoms have subsided. His FEV1/FVC ratio is < 0.70, and FEV1 is 40% of predicted. What is the most likely finding that can be discovered from the histology of his bronchi?
A 59-year-old man comes to the physician because of a 1-year history of progressive shortness of breath and nonproductive cough. Pulmonary examination shows bibasilar inspiratory crackles. An x-ray of the chest shows multiple nodular opacities in the upper lobes and calcified hilar nodules. Pulmonary functions tests show an FEV1:FVC ratio of 80% and a severely decreased diffusing capacity for carbon monoxide. A biopsy specimen of a lung nodule shows weakly birefringent needles surrounded by concentric layers of hyalinized collagen. The patient has most likely been exposed to which of the following?
Practice by Chapter
Atelectasis
Practice Questions
Pulmonary edema
Practice Questions
Acute respiratory distress syndrome
Practice Questions
Obstructive lung diseases (emphysema, bronchitis)
Practice Questions
Asthma pathology
Practice Questions
Bronchiectasis
Practice Questions
Restrictive lung diseases
Practice Questions
Interstitial lung diseases
Practice Questions
Pulmonary vascular disorders
Practice Questions
Pulmonary infections
Practice Questions
Lung tumors (primary and metastatic)
Practice Questions
Pleural diseases
Practice Questions
Congenital lung anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app