
Neuropathology — MCQs

On this page
A 65-year-old man presents with progressive bradykinesia, resting tremor, and cogwheel rigidity. Within 6 months of initial motor symptom onset, he develops visual hallucinations and fluctuating cognition. He dies 8 years after symptom onset. Autopsy shows depigmentation of substantia nigra, and microscopy reveals eosinophilic cytoplasmic inclusions in neurons that are immunoreactive for alpha-synuclein. These inclusions are also found in the cortex. What is the most likely diagnosis?
A 28-year-old woman presents with vision loss in her right eye and numbness in her left leg that resolved spontaneously over 2 weeks. MRI shows multiple periventricular white matter lesions perpendicular to the lateral ventricles (Dawson fingers). Lumbar puncture reveals oligoclonal bands and elevated IgG index. Which pathologic finding would be expected on brain biopsy?
A 72-year-old man with a history of chronic hypertension presents with sudden onset right hemiparesis and aphasia. CT scan shows a hyperdense lesion in the left basal ganglia with surrounding edema and mass effect. He dies 48 hours later. Autopsy reveals a cavity filled with blood clot and hemosiderin-laden macrophages. Which vessels were most likely affected?
A 45-year-old woman presents with progressive weakness, ataxia, and dementia over 6 months. MRI shows diffuse cortical atrophy and T2 hyperintensities in the basal ganglia. EEG demonstrates periodic sharp wave complexes. CSF analysis shows elevated 14-3-3 protein and normal cell count. Brain biopsy reveals spongiform changes and no inflammation. What is the most likely underlying pathogenic mechanism?
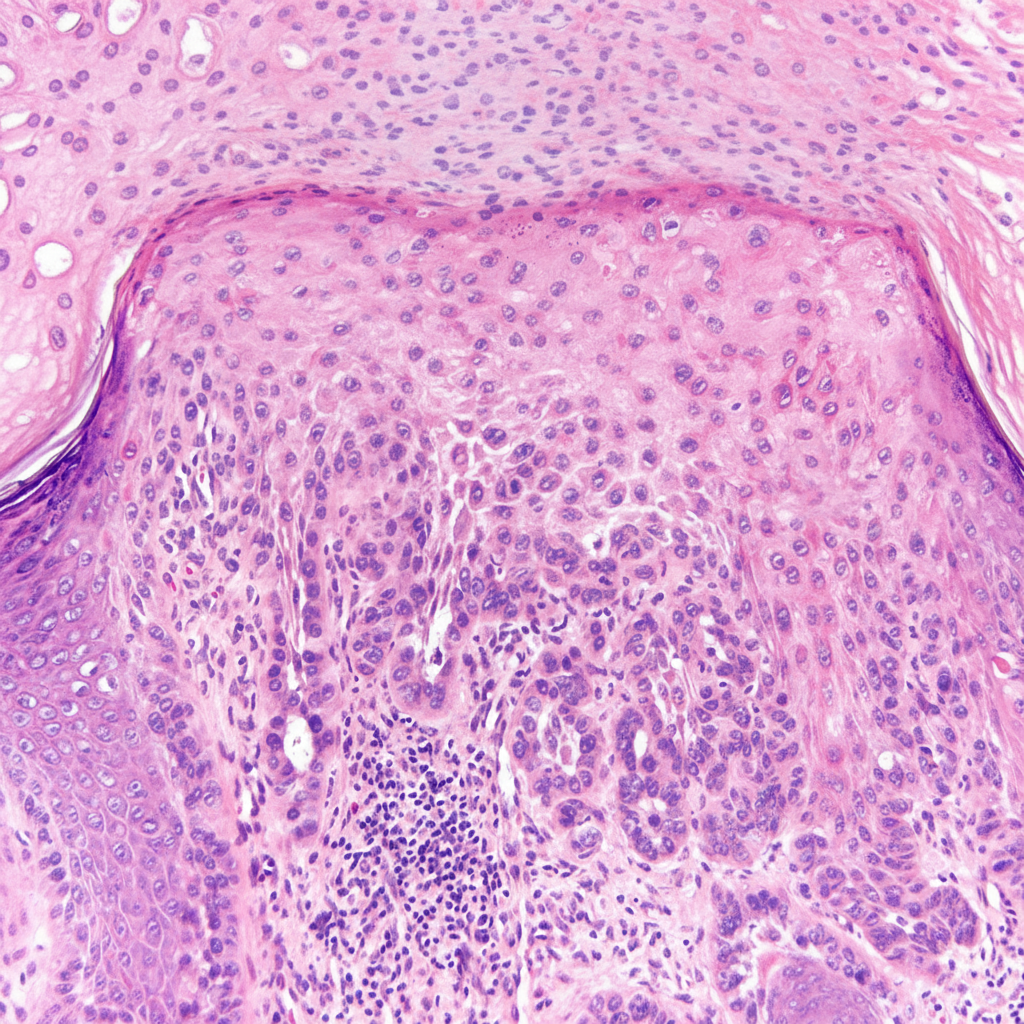
The following histological biopsy image shows presence of:
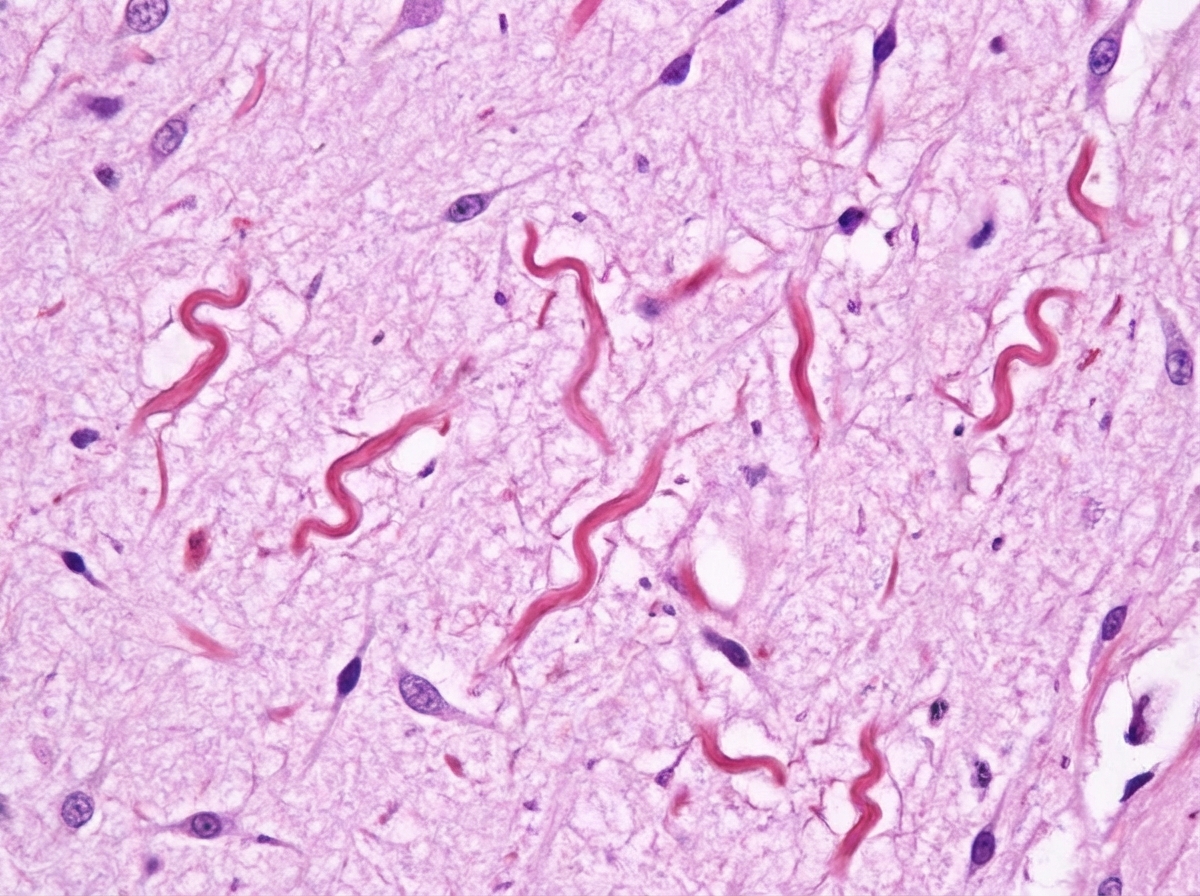
Cork screw inclusion bodies in brain biopsy specimen are seen in:
A 5-year-old child presented with gait ataxia and tremors in left hand. The image shows:
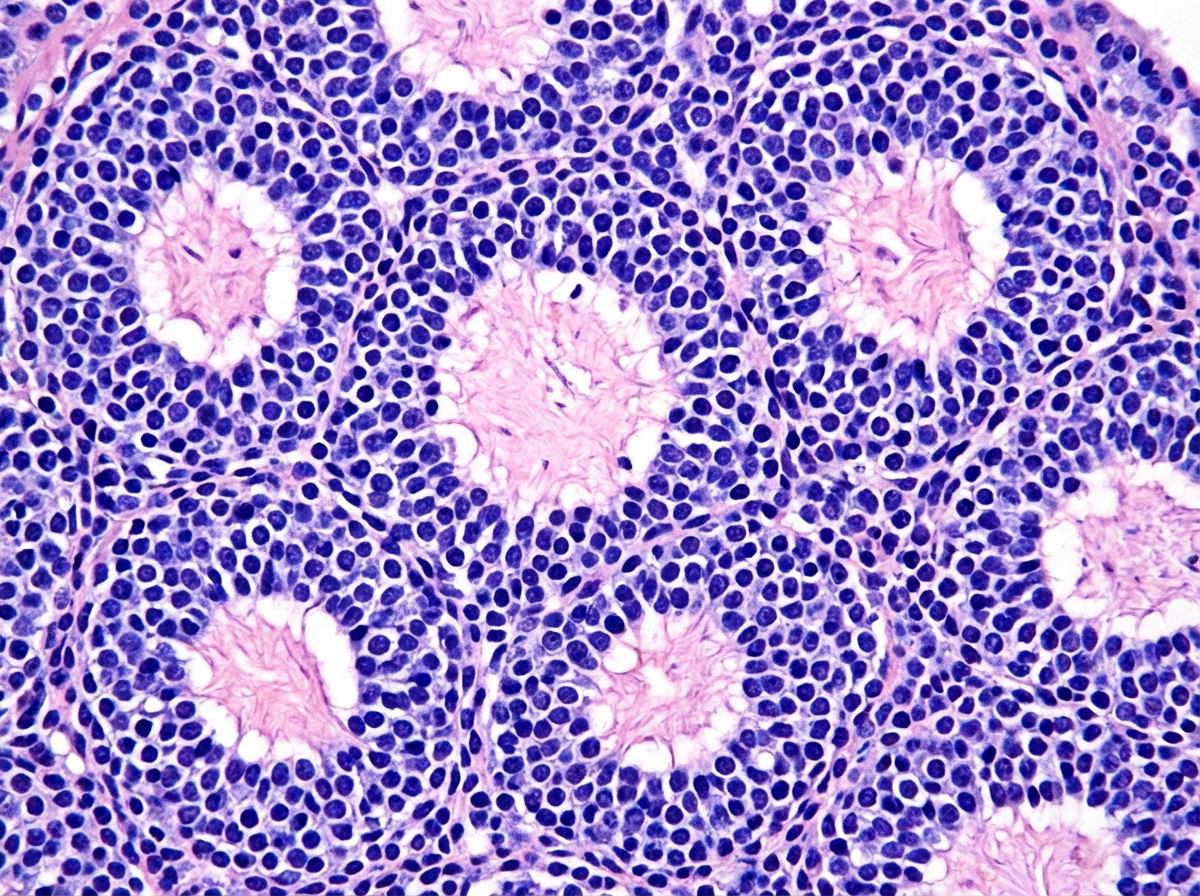
All are true about the brain tumour associated with the below mentioned histopathological findings except:
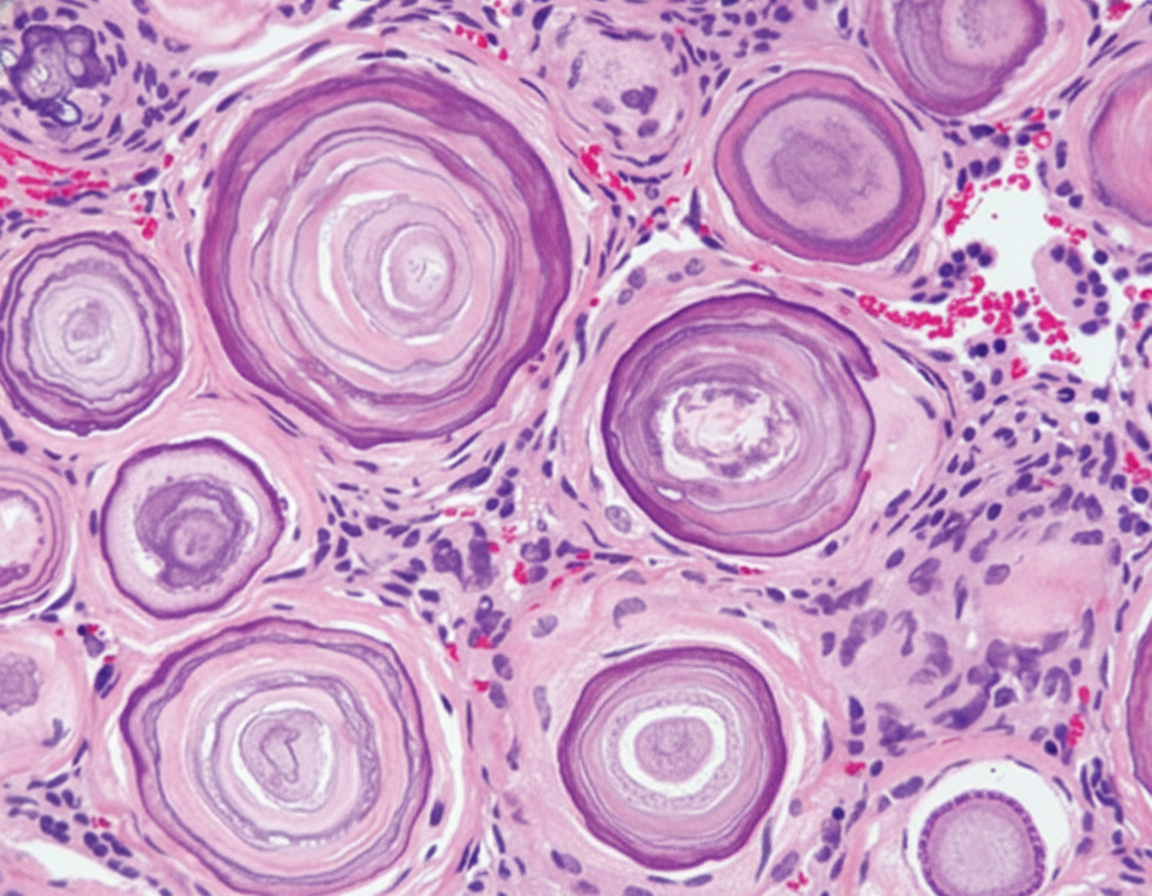
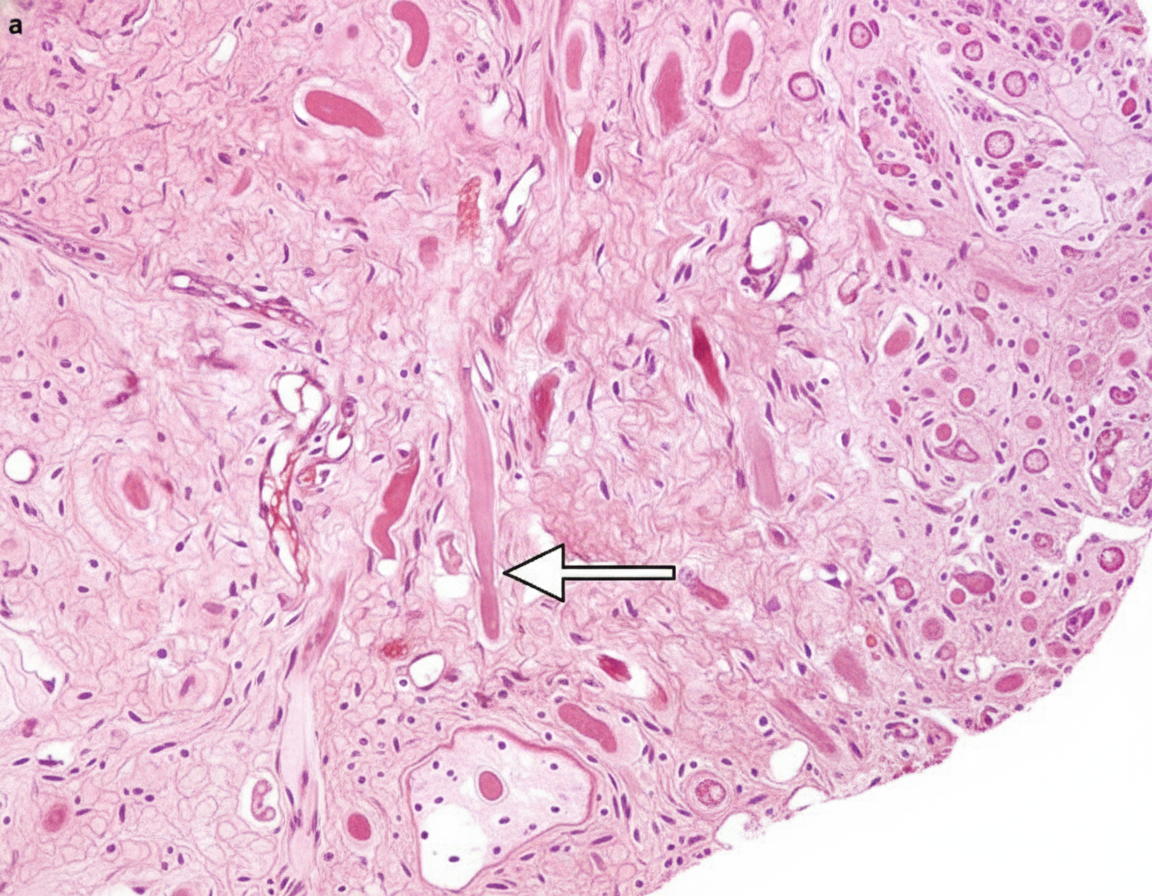
The following microscopic appearance is that of a schwannoma which most commonly involves the cerebellopontine angle. What does the area marked with the arrow represent?
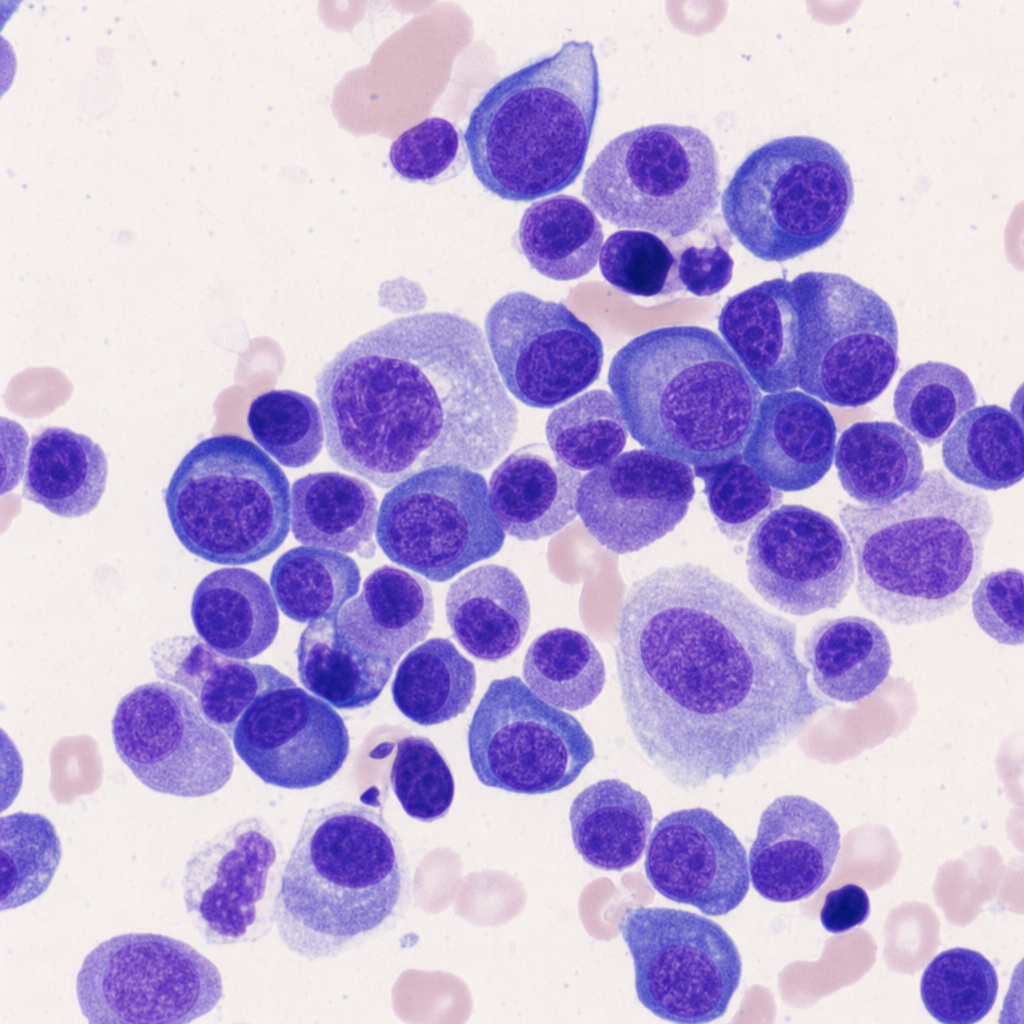
A biopsy from a solitary vertebral mass in a patient with no evidence of systemic disease shows the following cell. The mass is composed entirely of these cells, which show light-chain restriction on immunohistochemistry. This cell is the hallmark of:
Practice by Chapter
Cerebrovascular diseases
Practice Questions
CNS trauma
Practice Questions
CNS infections
Practice Questions
Demyelinating diseases
Practice Questions
Neurodegenerative diseases
Practice Questions
Alzheimer's disease pathology
Practice Questions
Parkinson's disease pathology
Practice Questions
Amyotrophic lateral sclerosis
Practice Questions
Primary CNS tumors
Practice Questions
Metastatic CNS tumors
Practice Questions
Peripheral nerve disorders
Practice Questions
Skeletal muscle diseases
Practice Questions
Congenital CNS malformations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app