
Demyelinating diseases — MCQs

A 32-year-old woman presents with a 3-month history of intermittent blurred vision and problems walking. The patient states that she often feels “pins and needles” in her legs that cause her problems when she’s walking. The patient is afebrile, and her vital signs are within normal limits. An autoimmune disorder is suspected. Which of the following findings would most likely be present in this patient?
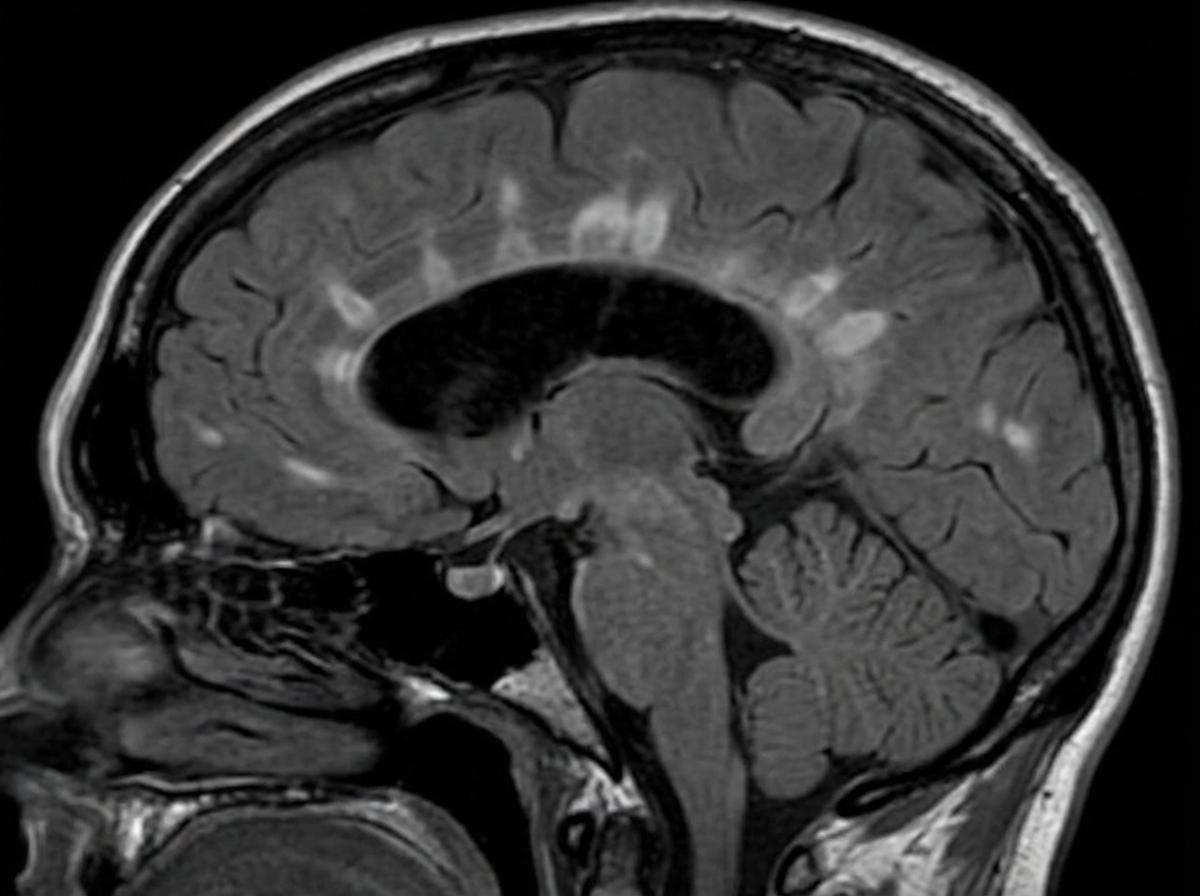
A 29-year-old woman presents with progressive vision loss in her right eye and periorbital pain for 5 days. She says that she has also noticed weakness, numbness, and tingling in her left leg. Her vital signs are within normal limits. Neurological examination shows gait imbalance, positive Babinski reflexes, bilateral spasticity, and exaggerated deep tendon reflexes in the lower extremities bilaterally. FLAIR MRI is obtained and is shown in the image. Which of the following is the most likely cause of this patient’s condition?
An 80-year-old woman is brought to the physician by her 2 daughters for worsening memory loss. They report that their mother is increasingly forgetful about recent conversations and events. She is unable to remember her appointments and commitments she has made. 3 years ago, the patient was moved into an elder care facility because she was often getting lost on her way home and forgetting to take her medications. The patient reports that she is very socially active at her new home and has long conversations with the other residents about her adventures as an air hostess during her youth. Which of the following cerebral pathologies is most likely present in this patient?
A 63-year-old man presents to the clinic concerned about numbness and weakness in his bilateral shoulders and arms for the past 8 weeks. The symptoms started when he fell from scaffolding at work and landed on his back. Initial workup was benign and he returned to normal duty. However, his symptoms have progressively worsened since the fall. He denies fever, back pain, preceding vomiting, and diarrhea. He has a history of type 2 diabetes mellitus, hypertension, hypercholesterolemia, ischemic heart disease, and a 48-pack-year cigarette smoking history. He takes atorvastatin, hydrochlorothiazide, lisinopril, labetalol, and metformin. His blood pressure is 132/82 mm Hg, the pulse is 72/min, and the respiratory rate is 15/min. All cranial nerves are intact. Muscle strength is reduced in the upper limbs (4/5 bilaterally) but normal in the lower limbs. Perception of sharp stimuli and temperature is reduced on his shoulders and upper arms. The vibratory sense is preserved. Sensory examination is normal in the lower limbs. What is the most likely diagnosis?
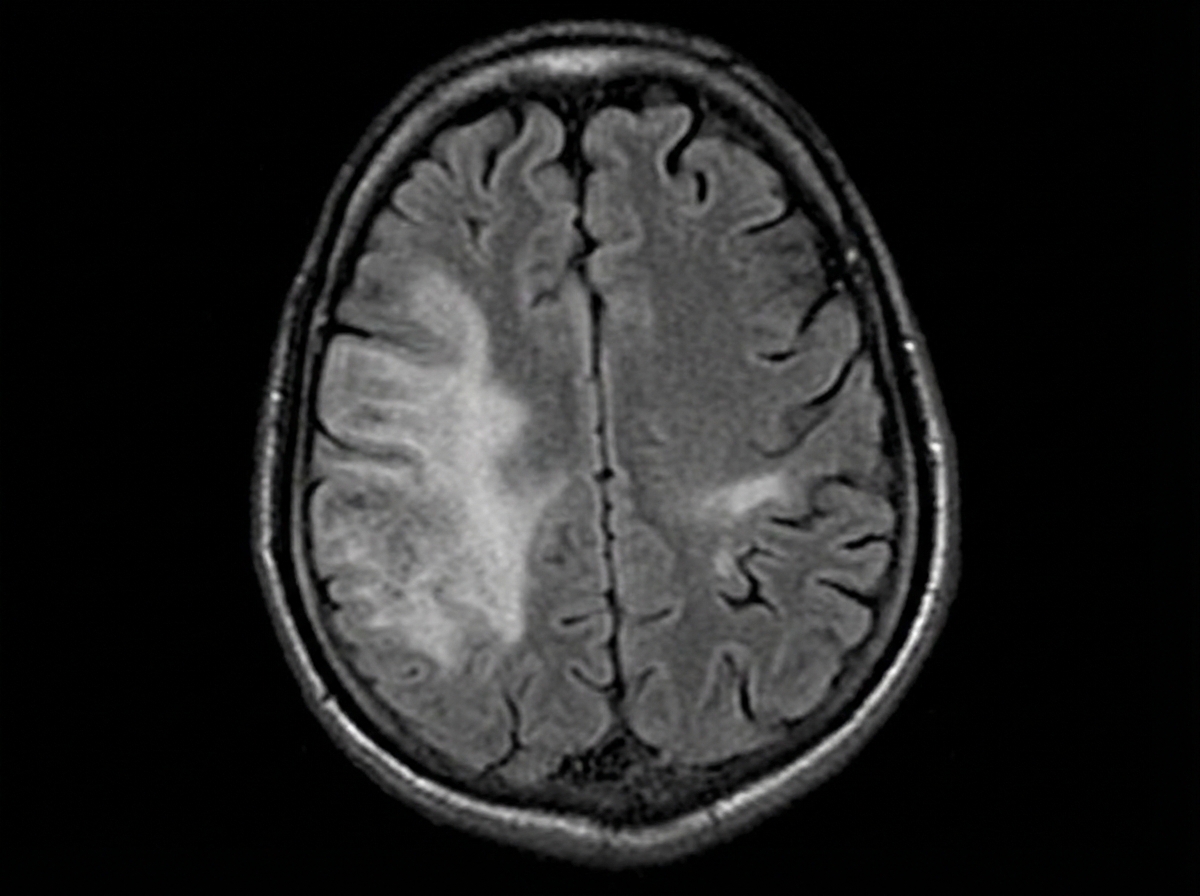
A 35-year-old woman with a history of Crohn disease presents for a follow-up appointment. She says that lately, she has started to notice difficulty walking. She says that some of her friends have joked that she appears to be walking as if she was drunk. Past medical history is significant for Crohn disease diagnosed 2 years ago, managed with natalizumab for the past year because her intestinal symptoms have become severe and unresponsive to other therapies. On physical examination, there is gait and limb ataxia present. Strength is 4/5 in the right upper limb. A T1/T2 MRI of the brain is ordered and is shown. Which of the following is the most likely diagnosis?
A 38-year-old woman comes to the physician for a follow-up examination. Two years ago, she was diagnosed with multiple sclerosis. Three weeks ago, she was admitted and treated for right lower leg weakness with high-dose methylprednisone for 5 days. She has had 4 exacerbations over the past 6 months. Current medications include interferon beta and a multivitamin. Her temperature is 37°C (98.6°F), pulse is 90/min, and blood pressure is 116/74 mm Hg. Examination shows pallor of the right optic disk. Neurologic examination shows no focal findings. She is anxious about the number of exacerbations and repeated hospitalizations. She is counseled about the second-line treatment options available to her. She consents to treatment with natalizumab. However, she has read online about its adverse effects and is concerned. This patient is at increased risk for which of the following complications?
A 28-year-old man presents to the emergency department with lower extremity weakness. He was in his usual state of health until 10 days ago. He then began to notice his legs were “tiring out” during his workouts. This progressed to difficulty climbing the stairs to his apartment. He has asthma and uses albuterol as needed. He has no significant surgical or family history. He smokes marijuana daily but denies use of other recreational drugs. He is sexually active with his boyfriend of 2 years. He has never traveled outside of the country but was camping 3 weeks ago. He reports that he had diarrhea for several days after drinking unfiltered water from a nearby stream. On physical examination, he has 1/5 strength in his bilateral lower extremities. He uses his arms to get up from the chair. Achilles and patellar reflexes are absent. A lumbar puncture is performed, and results are as shown below: Cerebral spinal fluid: Color: Clear Pressure: 15 cm H2O Red blood cell count: 0 cells/µL Leukocyte count: 3 cells/ µL with lymphocytic predominance Glucose: 60 mg/dL Protein: 75 mg/dL A culture of the cerebral spinal fluid is pending. Which of the following is the part of the management for the patient’s most likely diagnosis?
A 43-year-old man presents to the emergency department following a work-related accident in which both arms were amputated. The patient lost a substantial amount of blood prior to arrival, and his bleeding is difficult to control due to arterial damage and wound contamination with debris. His complete blood count (CBC) is significant for a hemoglobin (Hgb) level of 5.3 g/dL. The trauma surgery resident initiates the massive transfusion protocol and orders whole blood, O negative, which she explains is the universal donor. The patient receives 6 units of O negative blood prior to admission. He subsequently develops fever, chills, hematuria, and pulmonary edema. Several hours later, the patient goes into hemodynamic shock requiring the emergent administration of vasopressors. Of the following options, which hypersensitivity reaction occurred?
A 67-year-old woman comes to the physician because of a 3-week history of fatigue and worsening back and abdominal pain. During this period, she has also had excessive night sweats and a 4.6-kg (10-lb) weight loss. She has had swelling of the neck for 3 days. She does not smoke or drink alcohol. Vital signs are within normal limits. Physical examination shows a 4-cm, supraclavicular, nontender, enlarged and fixed lymph node. The spleen is palpated 2 cm below the left costal margin. Laboratory studies show: Hemoglobin 10.4 g/dL Mean corpuscular volume 87 μm3 Leukocyte count 5,200/mm3 Platelet count 190,000/mm3 Serum Lactate dehydrogenase 310 U/L A CT scan of the thorax and abdomen shows massively enlarged paraaortic, axillary, mediastinal, and cervical lymph nodes. Histopathologic examination of an excised cervical lymph node shows lymphocytes with a high proliferative index that stain positive for CD20. Which of the following is the most likely diagnosis?
A 61-year-old woman comes to the physician because of a constant, dull headache and generalized body pains for the past 8 months. She has also had difficulty hearing from her left side, which started a month after the onset of the headaches. Five months ago, she had surgery to correct a fracture of the right femur that occurred without a fall or any significant trauma. Five years ago, she underwent a total thyroidectomy for localized thyroid carcinoma. She takes levothyroxine and calcium supplements, which she started after menopause. Physical examination reveals a prominent forehead and irregular, tender skull surface. Bony tenderness is present over bilateral hip and knee joints, with decreased range of motion of the right hip joint and increased anterior curvature of both tibias. Laboratory studies show a highly elevated level of alkaline phosphatase, with vitamin D, calcium and PTH levels within normal limits. A plain x-ray of the head is most likely to show which of the following findings?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app